CASE20240702_001
OCT Guided Angioplasty of Severe Ostial Circumflex Lesion Through Previously Deployed Old LAD Stent
By Saurabh Goel, Ashish Goel
Presenter
Saurabh Goel
Authors
Saurabh Goel1, Ashish Goel2
Affiliation
Wockhardt Hopsital, Mumbai Central, India1, Fayth Clinic, Mumbai, India2,
View Study Report
CASE20240702_001
Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
OCT Guided Angioplasty of Severe Ostial Circumflex Lesion Through Previously Deployed Old LAD Stent
Saurabh Goel1, Ashish Goel2
Wockhardt Hopsital, Mumbai Central, India1, Fayth Clinic, Mumbai, India2,
Clinical Information
Relevant Clinical History and Physical Exam
A 70-year-old hypertensive male, non-diabetic, presented with new-onset angina on moderate exertion for 15 days. He underwent PTCA to LAD in 2010 with a 3x38mm Xience Prime stent. He does not use tobacco and takes aspirin 150mg, atorvastatin 40mg, telmisartan 40mg, and metoprolol 50mg regularly. His LV ejection fraction was 55% on a 2D Echo three months ago, with no prior symptoms. Clinical examination showed HR 68/min, BP 126/86 mmHg, and normal cardiovascular and respiratory findings.
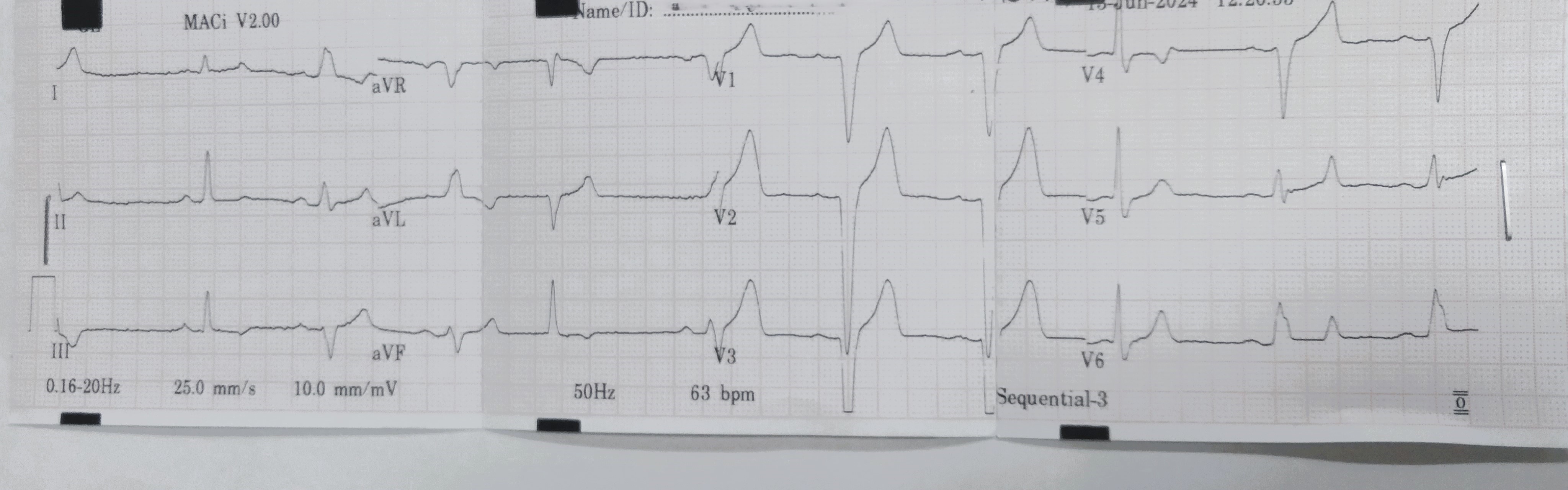
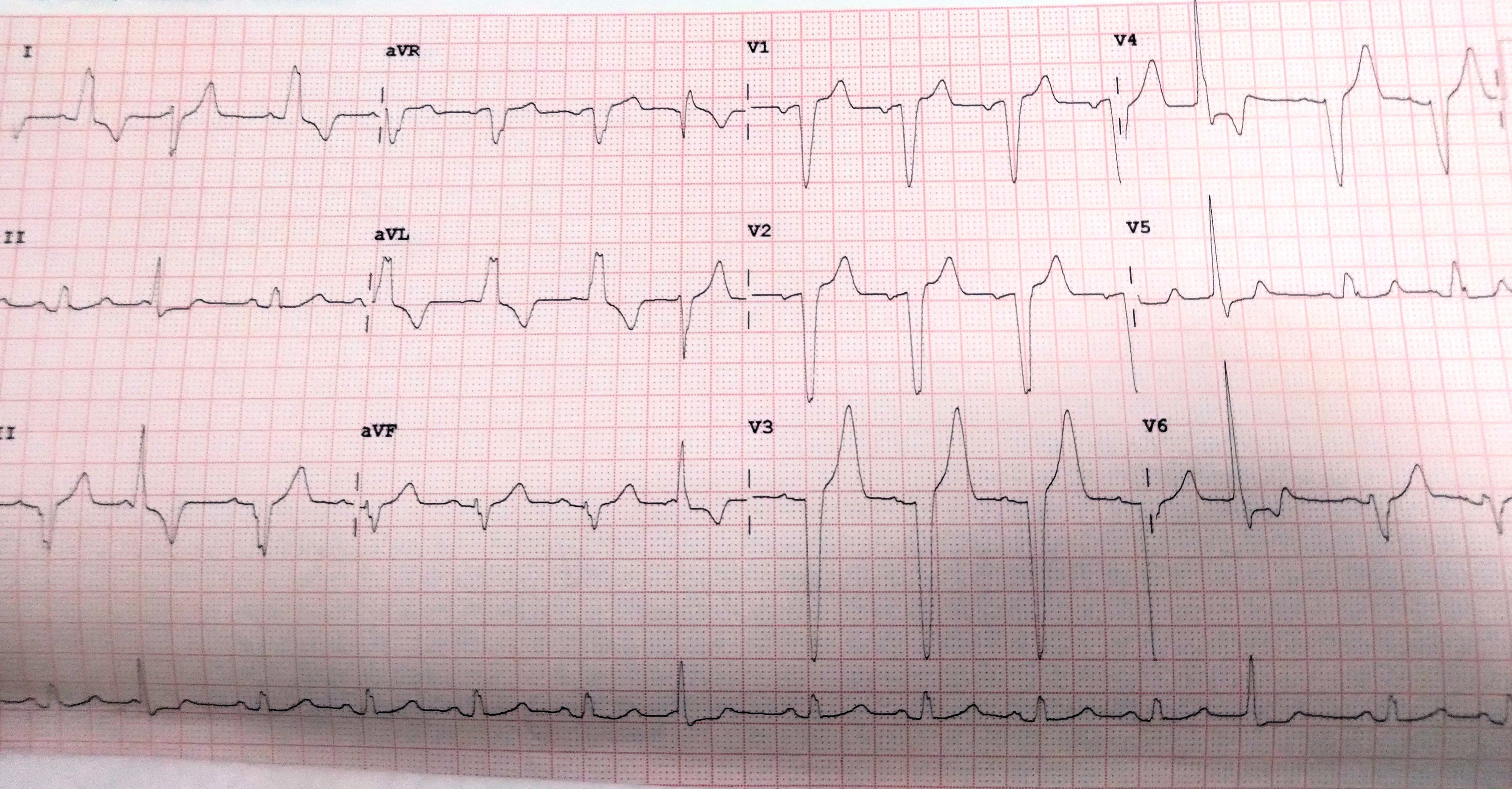
Relevant Test Results Prior to Catheterization
ECG showed LBBB pattern with frequent ventricular ectopics. 2D echocardiography, previously showing an LV ejection fraction of 55%, now showed a reduction to 45%, with jerky motion of the proximal septum and marked hypokinesia of apicolateral segments, and diastolic dysfunction. His renal function and troponin I were normal. After optimizing medical therapy, he was taken for coronary angiography.

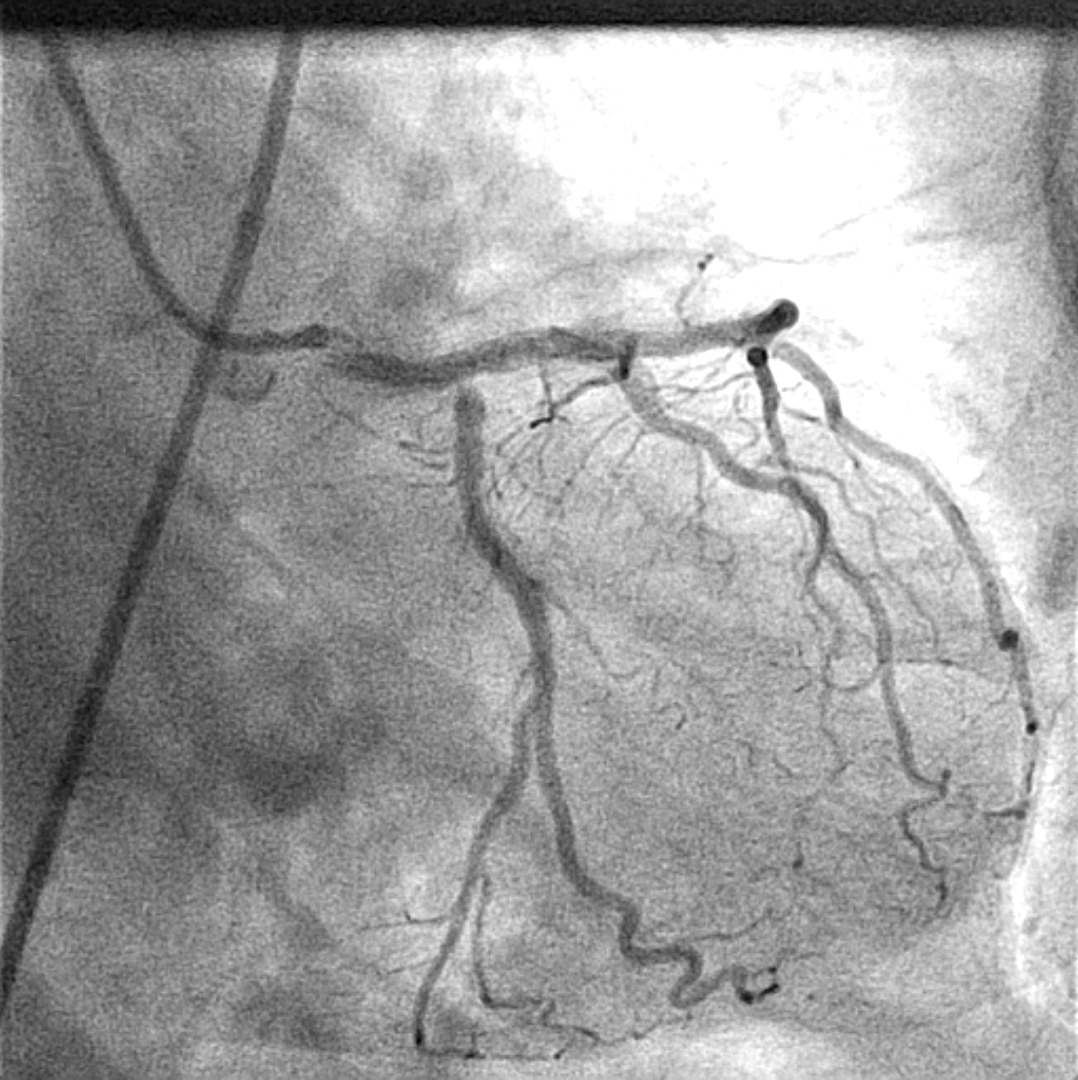
Relevant Catheterization Findings
The left main artery was normal. LAD showed a patent long stent from the ostium, placed across the left circumflex (LCX) ostium, with no restenosis. Severe ostial 95% stenosis of LCX was noted, which was a good sized non dominant vessel. The non-dominant right coronary artery had minor plaques. Due to the unstable presentation and severe ostial LCX lesion with a previous LAD stent across it, PTCA of LCX, using OCT guidance was decided.

 Catheterization Findings.mp4
Catheterization Findings.mp4
Interventional Management
Procedural Step
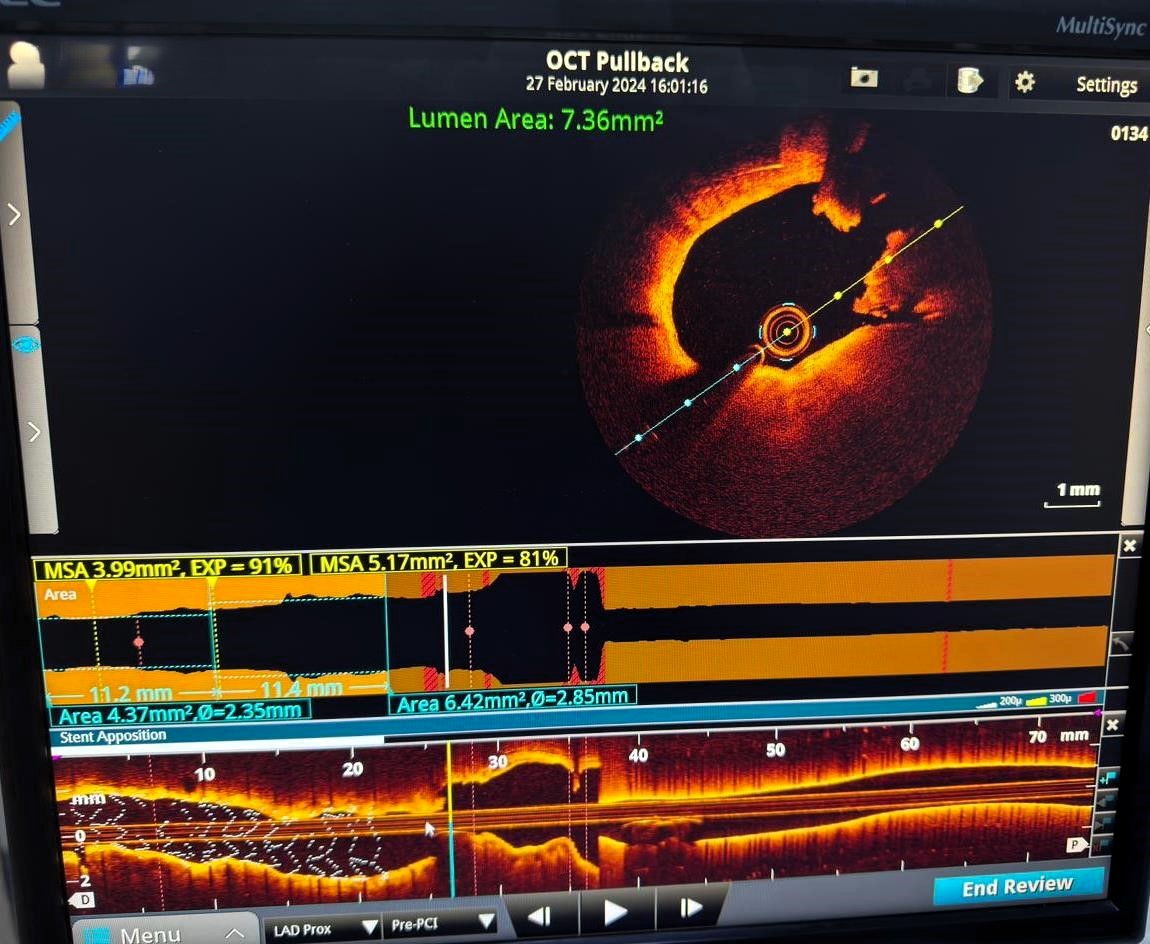
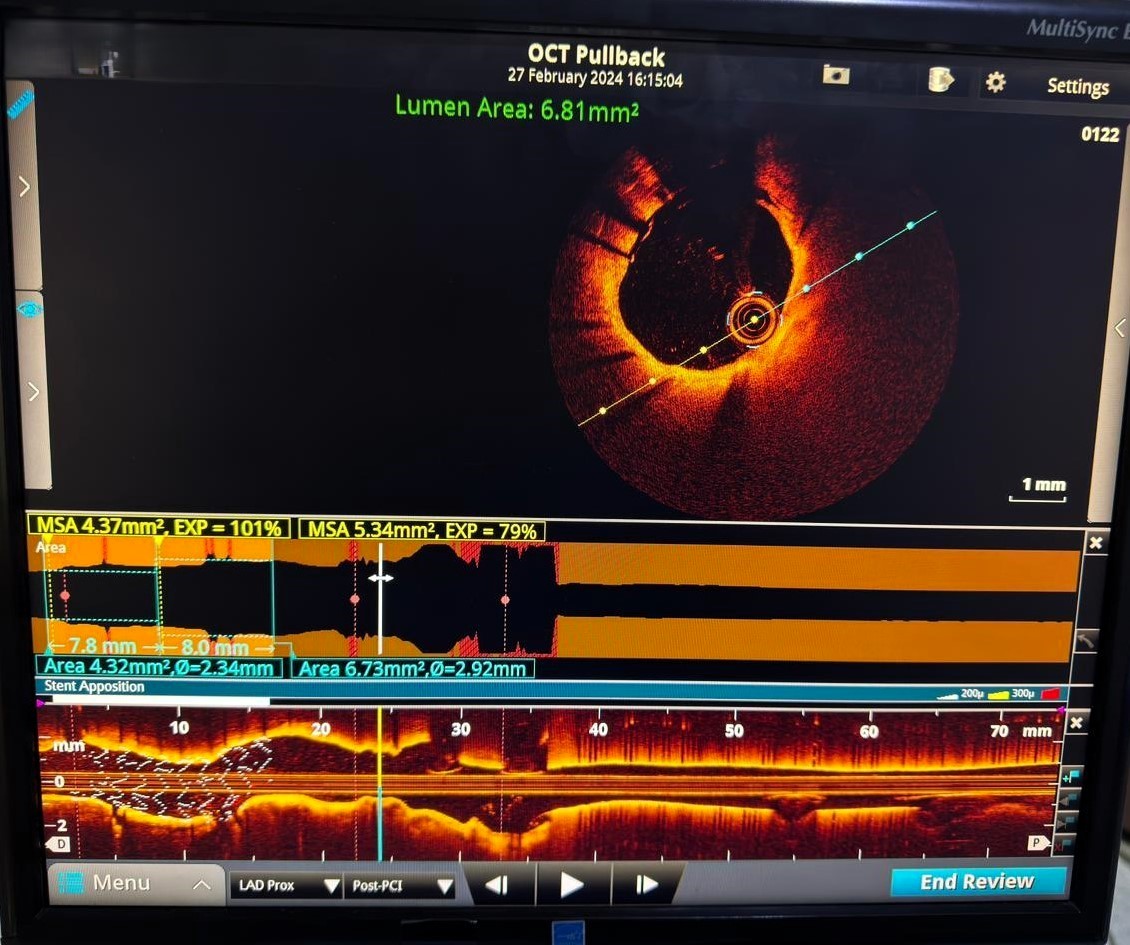
The left coronary artery was cannulated with a 7 F XB 3 guide. Turn Trak wires were placed in both LCX and LAD. The ostial LCX lesion was pre-dilated using a 2.5 x 12 mm NC Trek balloon. Subsequently, an OCT catheter was advanced to the LCX ostium, but due to the acute curve and a previous LAD stent, it could not advance into the LCX and was therefore placed in the distal LAD. A pullback OCT was performed from proximal LAD towards the ostium of the left main. OCT imaging revealed that the LAD stent was well endothelialized, and the ostium of the LCX exhibited a lipid-rich irregular lesion with marked dissection. Left main did not show any significant disease. A 2.75 x 12 mm Xience Alpine stent was introduced into the proximal LCX at the ostium, and a 2.75 x 12 mm NC Trek balloon was placed at the LAD ostium. After confirming the exact ostial position, the stent was deployed at the LCX ostium. The stent balloon was slightly advanced into the LCX and crushed with the 2.75 x 12 NC Trek balloon. The LCX stent balloon was then withdrawn just into the LAD ostium, and a kissing inflation was performed. Final OCT run showed the LCX stent was well placed with no protruding struts, a well-formed carina, and excellent final result.
Intervention.mp4
Case Summary
This case illustrates the challenging angioplasty of a severe ostial LCX lesion through a previous LAD stent. The presence of old stent struts, the lesion's location, and the acute angle of the LCX ostium significantly increased the procedure's complexity. Although a drug-coated balloon was considered, initial balloon dilation and OCT imaging revealed a complex dissected plaque, necessitating stenting. Precise stent placement and kissing balloon dilatation were performed, resulting in an excellent final outcome as confirmed by OCT. This case highlights the critical role of advanced imaging and meticulous techniques in managing complex coronary lesions effectively.