
CASE20220903_002
A Case Of Complex And High-Risk Coronary Intervention With Left Main Bifurcation Stenting
By ,
Presenter
Richardson Lorilla
Authors
1, 1
Affiliation
, Philippines1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
A Case Of Complex And High-Risk Coronary Intervention With Left Main Bifurcation Stenting
1, 1
, Philippines1
Clinical Information
Patient initials or Identifier Number
A.B.
Relevant Clinical History and Physical Exam
64 year old male with one year history of easy fatigability, chest discomfort and dyspnea on exertion. He consulted with a physician and requested for 2D echo showed abnormal results.
Known hypertensive and diabetic with 20 pack years smoking history and occasional alcoholic drinker.
Scheduled for elective coronary angiogram.
He came in with stable vital signs blood pressure 130/80 mmHg and pulse rate of 61 beats per minute.
His physical examination was unremarkable.
Known hypertensive and diabetic with 20 pack years smoking history and occasional alcoholic drinker.
Scheduled for elective coronary angiogram.
He came in with stable vital signs blood pressure 130/80 mmHg and pulse rate of 61 beats per minute.
His physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
2D echocardiogram showed ejection fraction of 22% with global hypokinesia.
creatinine 1.1 mg/dl egfr- 70
Sodium- 138 mmol
Potassium- 4.8 mmol
Hemoglobin 146hematocrit - 44platelet count 202
creatinine 1.1 mg/dl egfr- 70
Sodium- 138 mmol
Potassium- 4.8 mmol
Hemoglobin 146hematocrit - 44platelet count 202
Relevant Catheterization Findings
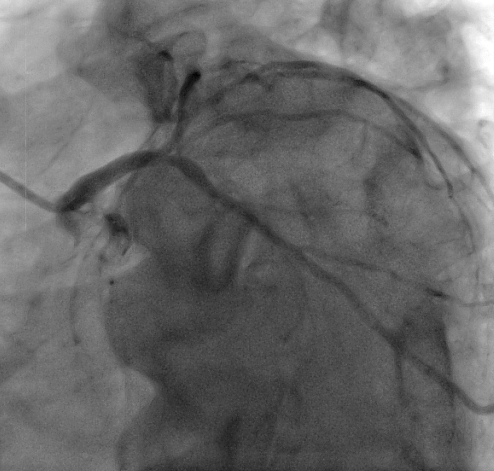
Patient was admitted and underwent coronary angiogram as elective procedure which revealed severe three vessel coronary artery disease with left main involvement.
LMCA- 40-50% distal segment stenosis
LAD- 70-80% postal segment stenosis with a hazy linear ulcerated plaque at its mid segment after the takeoff of the diagonal branch and another 90% mid segment stenosis
LCX- 80% postal segment stenosis and another 70% tubular segment stenosis
RCA- showed a RPLA with 70% concentric stenosis mid segment

 video A.avi
video A.avi
video B.avi
video C.avi
LMCA- 40-50% distal segment stenosis
LAD- 70-80% postal segment stenosis with a hazy linear ulcerated plaque at its mid segment after the takeoff of the diagonal branch and another 90% mid segment stenosis
LCX- 80% postal segment stenosis and another 70% tubular segment stenosis
RCA- showed a RPLA with 70% concentric stenosis mid segment
Interventional Management
Procedural Step
PTCA of the LMCA, LAD , LCx and RPLA was done via right radial access was done.
into the LCx and was parked distally.
Serial pre-stent dilatation of the proximal to mid LAD was done using an (Emerge) 1.5x20 mm PTCA balloon followed by (Euphora) 2.0 x 25 mm PTCA balloon.
A (Resolute Integrity)2.25x30mm DES was deployed at the mid LAD.
An (Ultimaster Tansei) 2.5x38mm DES was deployed at proximal to mid LCx.
A (Destiny) 3.5 x 23 mm DES was deployed at the LMCA to proximal LCx overlapping the previously deployed stent
A Supraflex 2.75 x16 mm DES was deployed at ostial segment of LAD overlapping the previously deployed stent at proximal LAD
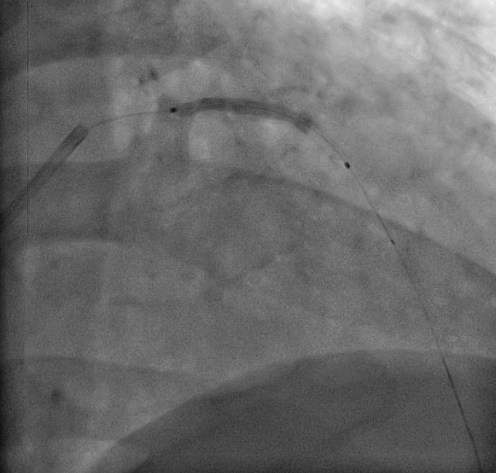
Simultaneous post stent balloon dilatation at the LAD and Lcx was done using a double kissing balloon technique.
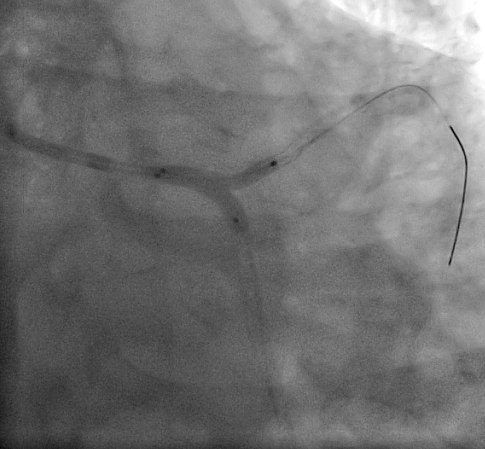
A JR 4 Fr. 6 guide catheter was used to cannulate the RCA. A Runthrough PTCA wire was parked distally into the RPLA. Pre-stent dilatation with an
(Accuforce) 2.75x15m. A (Destiny) 2.5 x 15 mm DES was deployed at the PLA.
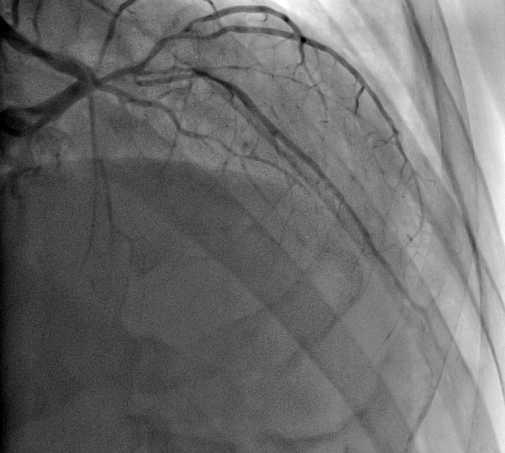
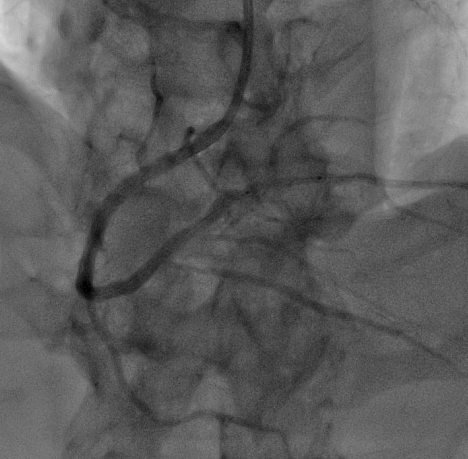
Final angiographic shots showed no loss of side branches, no residual stenosis and there was TIMI 3 flow.
Case Summary
Our patient is a 64 year old male, hypertensive, diabetic with a strong history of smoking. He underwent coronary angiogram due to 1 year history of chest discomfort, dyspnea on exertion, easy fatigability with 2DED findings of low EF at 22%. His angiogram showed severe 3 vessel disease with left main involvement. Initially appraised for nuclear imaging viability studies but opted to proceed with angioplasty on the same admission day. He underwent successful PTCA with bifurcation stenting of the LMCA, LAD and LCx and PTCA of the RPLA. Post procedure patient remained hemodynamically stable with no complications noted. Patient was then discharged improved and stable after 3 days of hospitalization.