
CASE20220826_023
Primary Retrograde Approach to Chronic Total Occlusion Percutaneous Coronary Intervention in a Patient With Both Subclavian Arteries Occlusion
By , , , , ,
Presenter
Ho Sung Jeon
Authors
1, 1, 1, 1, 1, 1
Affiliation
, Korea (Republic of)1
Complex PCI - Chronic Total Occlusion
Primary Retrograde Approach to Chronic Total Occlusion Percutaneous Coronary Intervention in a Patient With Both Subclavian Arteries Occlusion
1, 1, 1, 1, 1, 1
, Korea (Republic of)1
Clinical Information
Patient initials or Identifier Number
LCH
Relevant Clinical History and Physical Exam
A 66-year-old male, with diabetes mellitus, hypothyroidism and dyslipidemia came to hospital complaining of persistent dyspnea on exertion that lasted 1 year. He was non-smoker. Initial vital sign was as follows. The right arm blood pressure was 95/65 mmHg, and left arm blood pressure was 79/53 mmHg. There was a differnce in blood pressure between the arms.
Relevant Test Results Prior to Catheterization
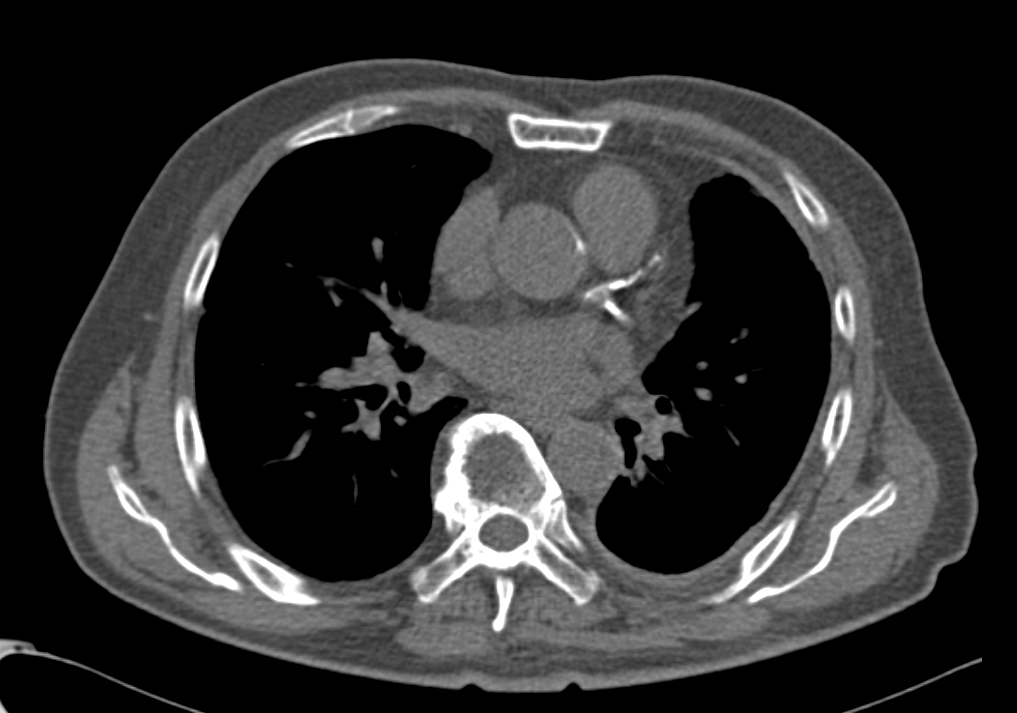
He had a chest computed tomography(CT) scan, and there was significant coronary artery calcification. Electrocardiogram(ECG) showed normal sinus rhythm. cardiac enzymes were within the normal range.Natriuretic peptide (NP) was also within the normal range.Transthoracic echocardiography(TTE) showed no regional wall motion abnormality and ejection fraction was preserved (58%).
Relevant Catheterization Findings
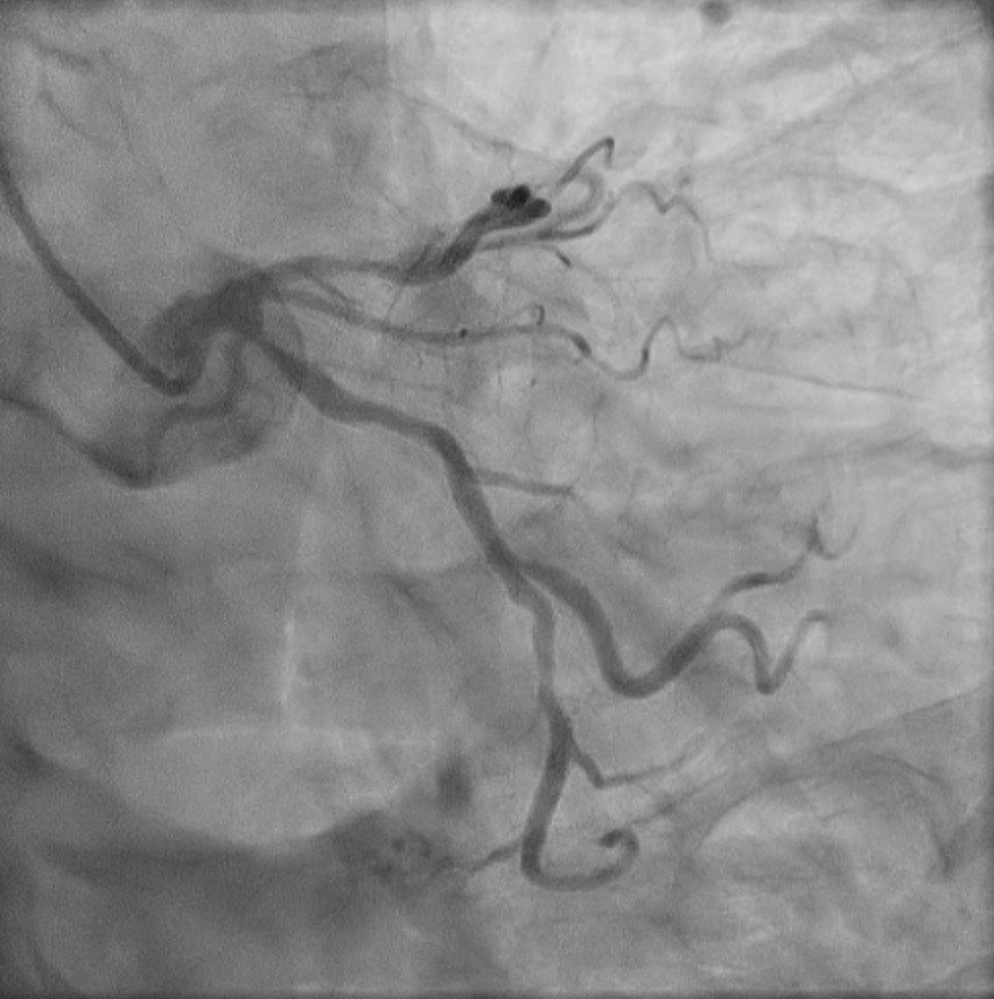
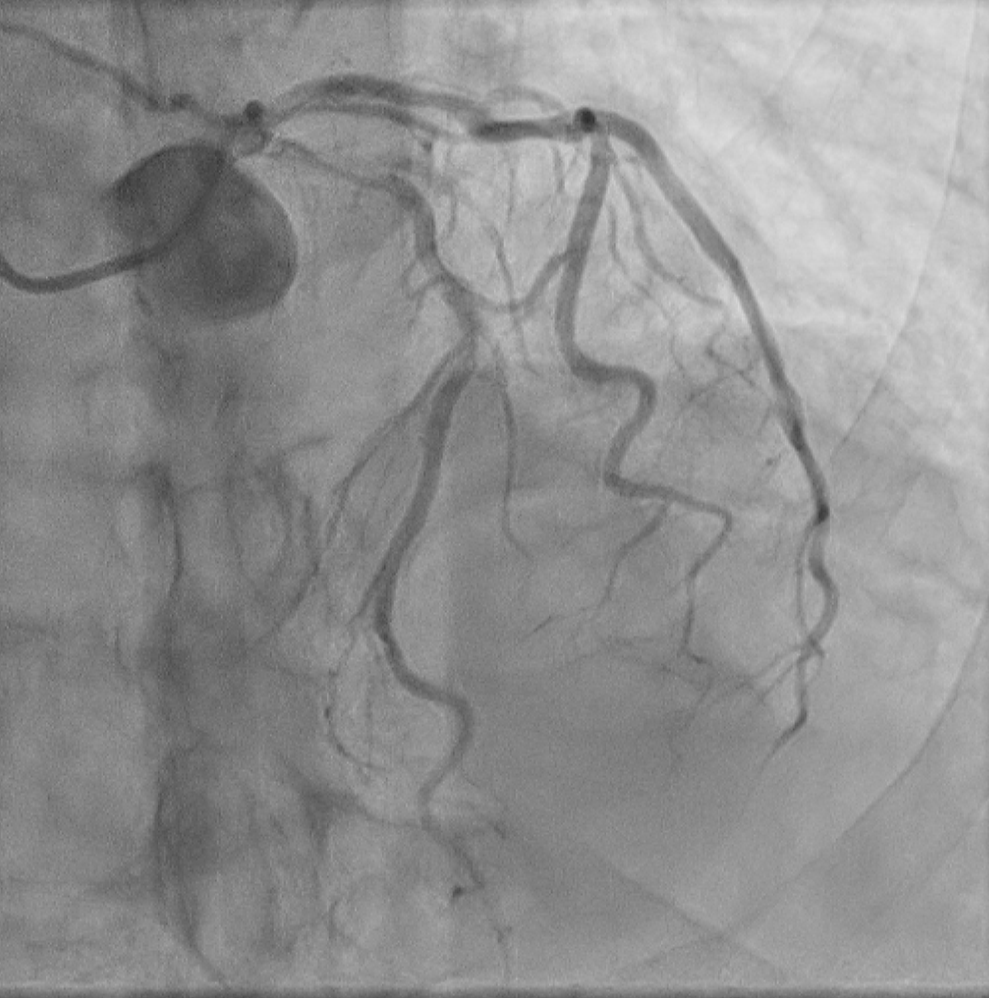
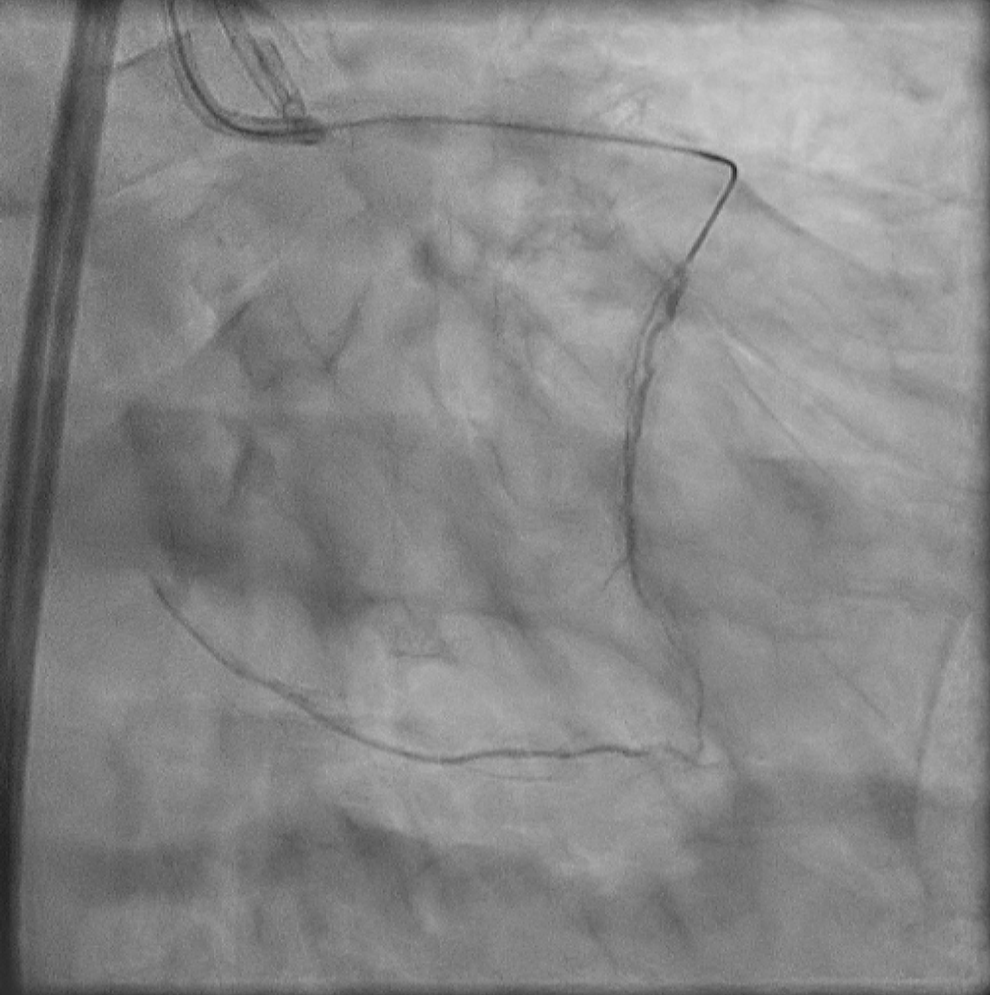
Coronary angiography (CAG) showed proximal right coronary artery (RCA) chronic total occlusion (CTO) withcontralateral collateral flow grade 2 from left anterior descending artery(LAD).Proximal LAD had diffuse irregular 80% stenosis with severe calcification and proximal left circumflex artery(LCX) had diffuse irregular 80% stenosis. with severe calcification.
 1.3.46.670589.29.1877192777354251330104228686519050630145814033.dcm.wmv
1.3.46.670589.29.1877192777354251330104228686519050630145814033.dcm.wmv
1.3.46.670589.29.1877192777354251330104241247255590630150019033.dcm.wmv
1.3.46.670589.29.1877192777354251330104245606657260630150101033.dcm.wmv
Interventional Management
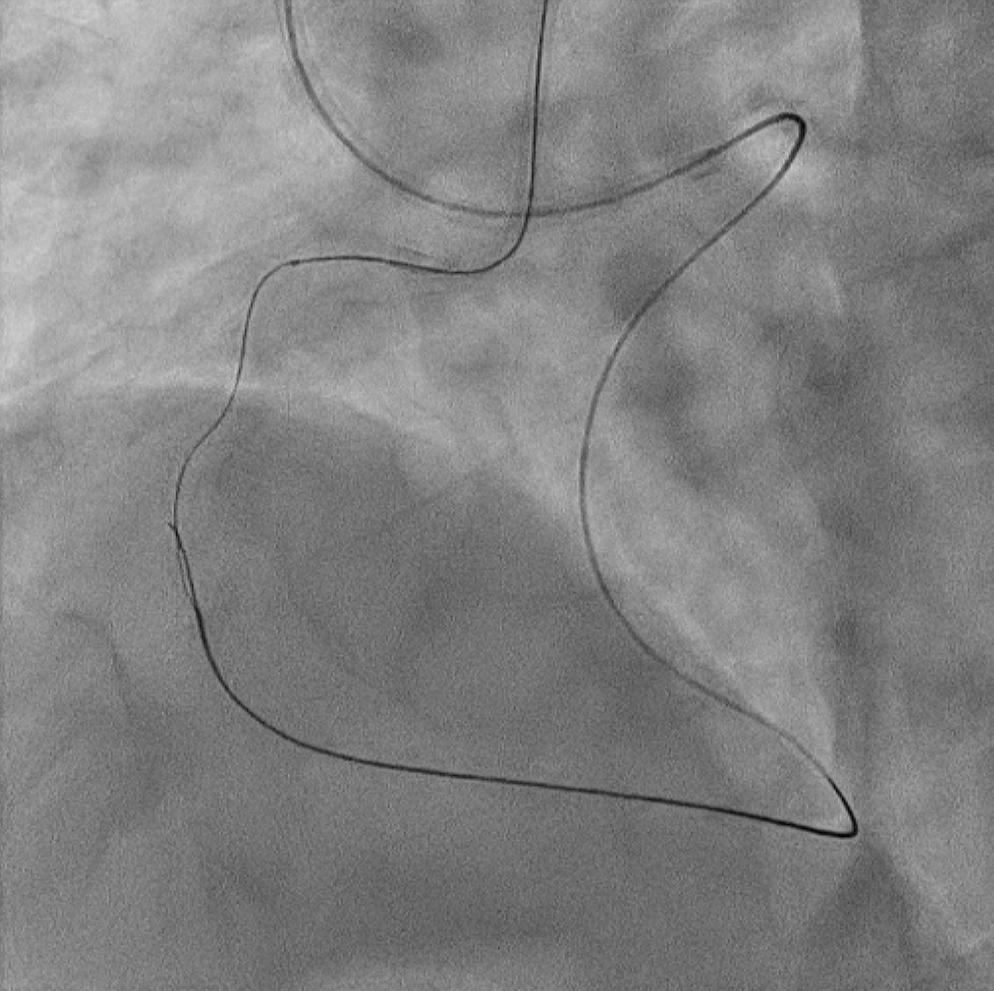
Procedural Step
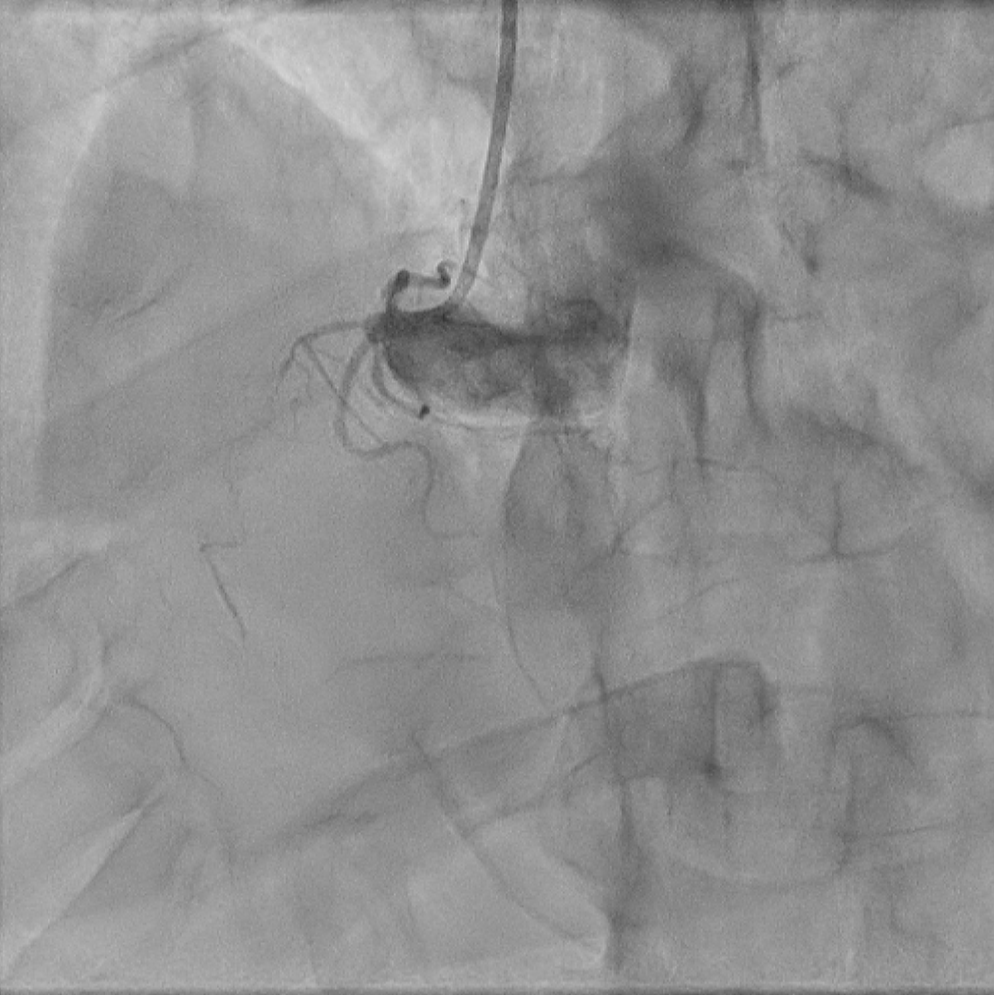
So we tried to check left internal mammaryartery(LIMA) due to possibility of coronary artery bypass graft(CABG). But leftsubclavian artery (SCA) total occlusion was seen. So we checked right internal mammary artery(RIMA). Right SCA also had significant stenosis.
1.3.46.670589.29.1877192777354251330155112964924510706121853033.dcm.wmv
1.3.46.670589.29.1877192777354251330155450941060210706131513033.dcm.wmv
1.3.46.670589.29.1877192777354251330155193980177020706123247033.dcm.wmv
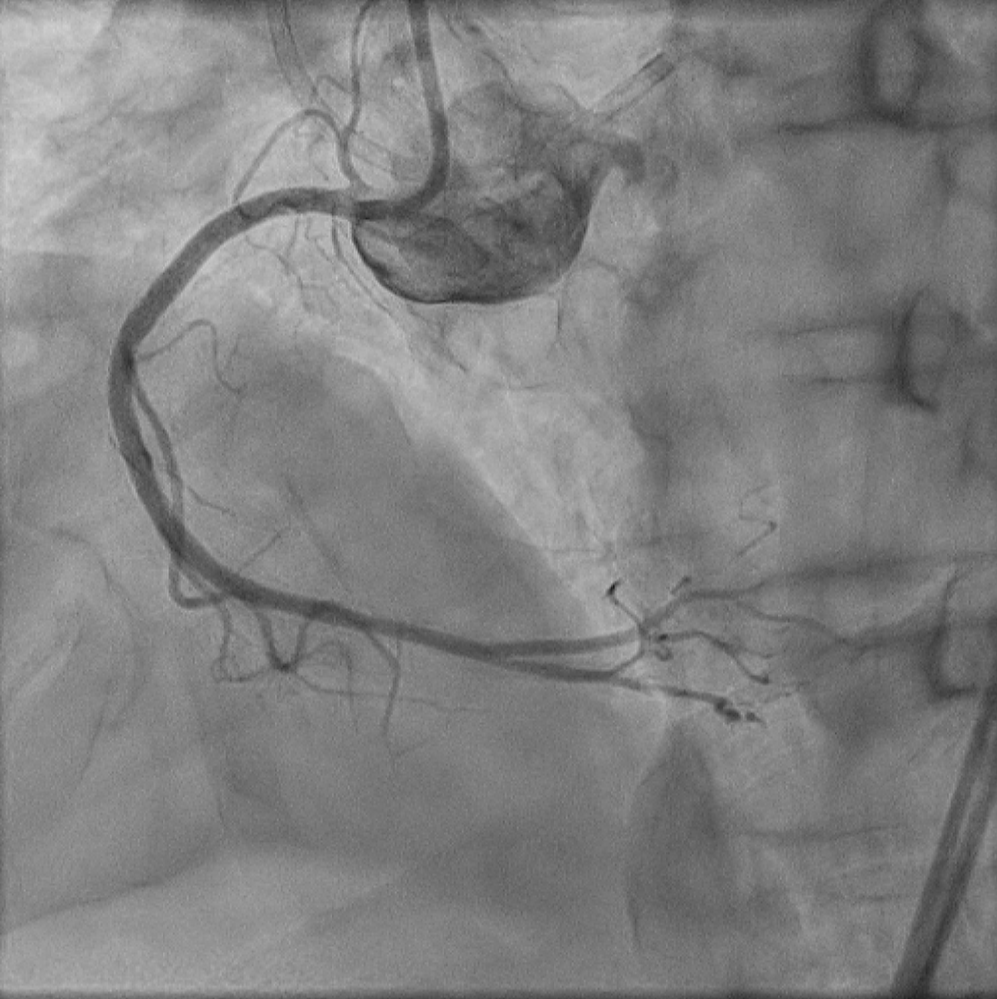
Case Summary
This is a case of successful hronic total occlusion(CTO) percutaneous coronary intervention(PCI) in a patient with both subclavian arteries stenosis who was not suitable for coronary artery bypass graft, and a case of successful primary retrograde CTO PCI with step by step.