
CASE20220826_022
Unexpected Complication, What To Do?
By
Presenter
Prashanth Panduranga
Authors
1
Affiliation
, Oman1
Complications - Complications
Unexpected Complication, What To Do?
1
, Oman1
Clinical Information
Patient initials or Identifier Number
ME
Relevant Clinical History and Physical Exam
• A53-year-old European male presented with effort angina class II, normal ECG andand positive exercise treadmill test. Non-diabetic and non-hypertensive. He hadCABG x 3 grafts in Europe 12 years earlier. Oneyear ago he underwent PCI to SVG to RCA 99% tight proximal lesion with a stentfor unstable angina presentation.
Relevant Test Results Prior to Catheterization
Normal routine blood tests. Negative Troponin T.LDL cholesterol was 3.4 mmol/L
Relevant Catheterization Findings
• From right femoral artery approach, there was tortuous iliac with difficulty in negotiating wire, hence JR4 catheter was taken with Terumo wire to cross right iliac artery and RCA injection was done first. RCA injection showed dominant right system with right coronary artery proximal 100% occluded. With the same JR diagnostic catheter grafts were injected which showed SVG to RCA 99% in-stent restenosis, SVG to OM stump.
Interventional Management
Procedural Step
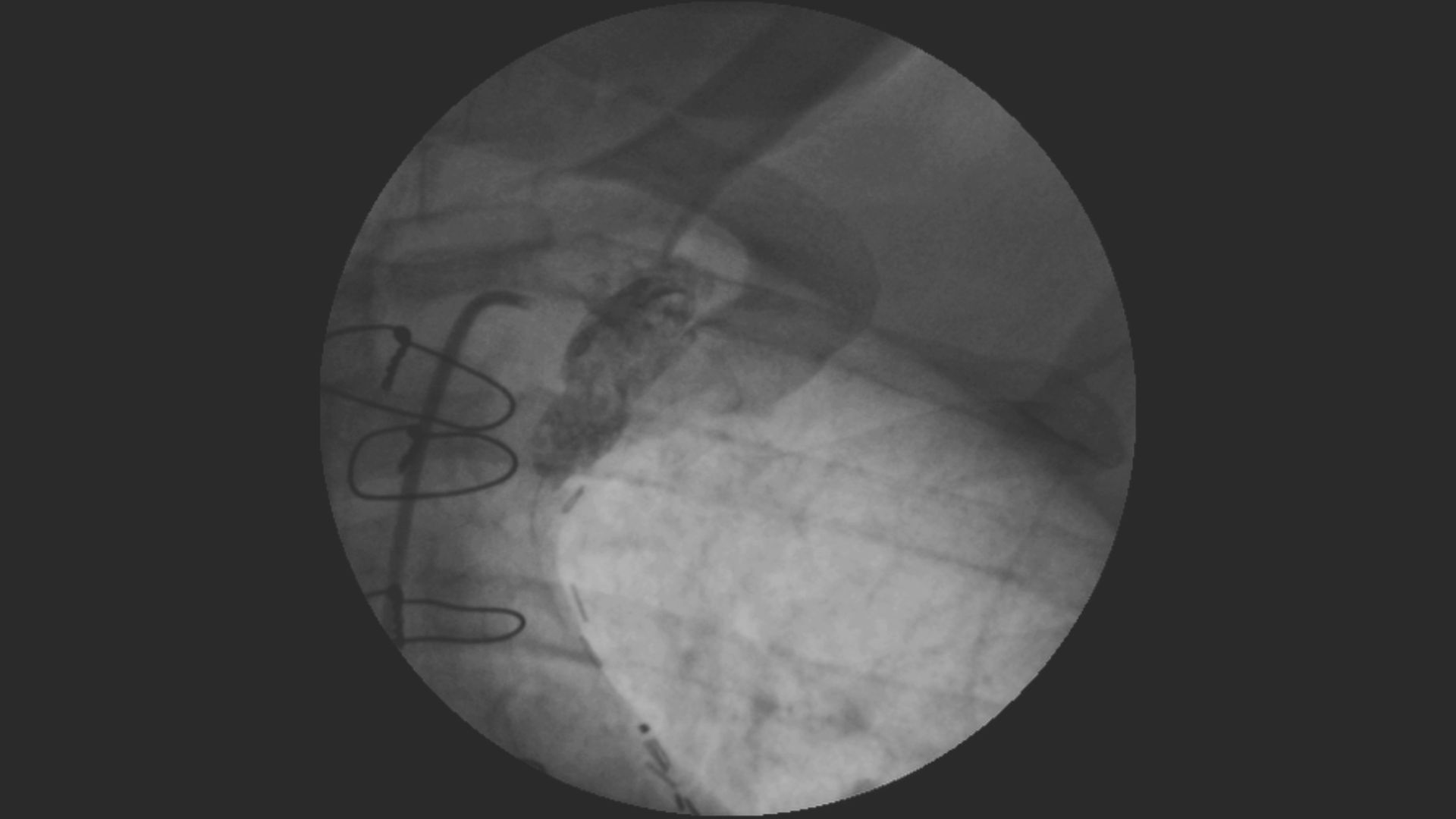
• As already JR catheter was in, LIMA cannulation was attempted. While attempting to cannulate LIMA using hydrophilic guide wire there was sudden appearance of dissection with huge dilatation of LIMA with no flow. Left subclavian artery no dissection was noted. However patient was hemodynamically stable with no chest pain or ECG changes. What to do now? With JL4 diagnostic catheter, LCA injection showed normal left main, left anterior descending artery in multiple views showed borderline lesion and the left circumflex artery 100% mid CTO.• Possible explanation for stability is that there was no significant left anterior artery disease, hence LIMA compromise did not lead to any ischemia. He was planned for PCI to SVG to RCA later. Manyinvestigators have reported discrepancies between the angiographic andfunctional severity of coronary angiographic stenosis. However, in dailypractice visual estimation of coronary stenosis is done followed byrevascularization. In astudy by Dogan et al (Int J Angiol. 2017 Mar; 26(1): 27–31.) among 886 coronaryangiographies of CABG patients, LIMA graft occlusion detected in 19 patient(2.1%), the LIMA-LAD competitive flow was found in 86 (9.7%) CABG patients. Theangiographic severity of the LAD stenosis in competitive flow group was mild in 20 (25%), moderate in 61 (70%), and severe coronary artery disease in 4 (5%)patients.

 Video 1.avi
Video 1.avi
Video 2.avi
Video 3.avi
Case Summary
Inconclusion, few unnecessary coronary stenting or CABG procedures are done due tolimited use of functional testing for clinical decision making. Hence this caseindicates the need for functional testing in borderline lesions beforerevascularization as recommended by current revascularization guidelines toprevent over diagnosis, misdiagnosis, or incorrect treatment decisions.