
CASE20220826_002
Coronary Arrtery Stent Removal
By
Presenter
Raman Chawla
Authors
1
Affiliation
, India1
Complications - Complications
Coronary Arrtery Stent Removal
1
, India1
Clinical Information
Patient initials or Identifier Number
xyz
Relevant Clinical History and Physical Exam
A 66years old female presented with c/o chest pain for duration of 1 day
Relevant Test Results Prior to Catheterization
Routine bloodinvestigations – Normal Troponin-T Positive Echo – Mild apical hypokinesia -EF 45% -No MR
Relevant Catheterization Findings
Interventional Management
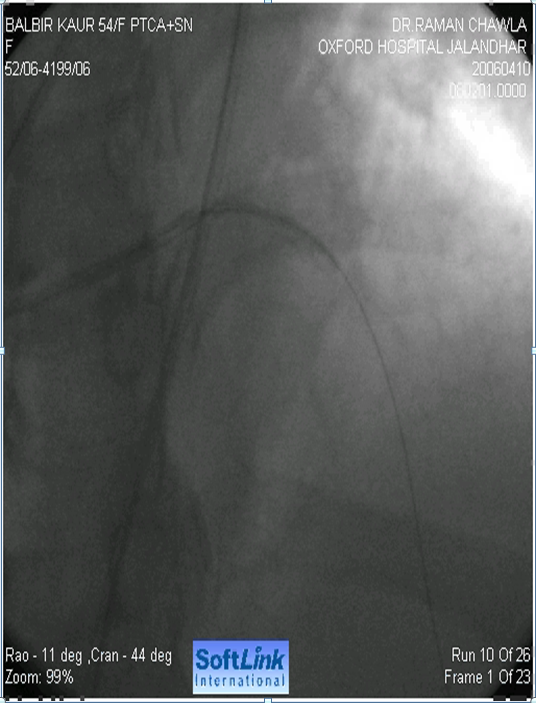
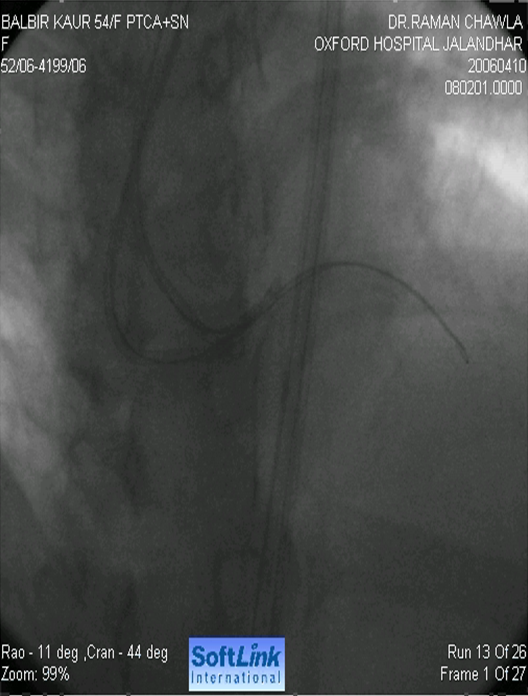
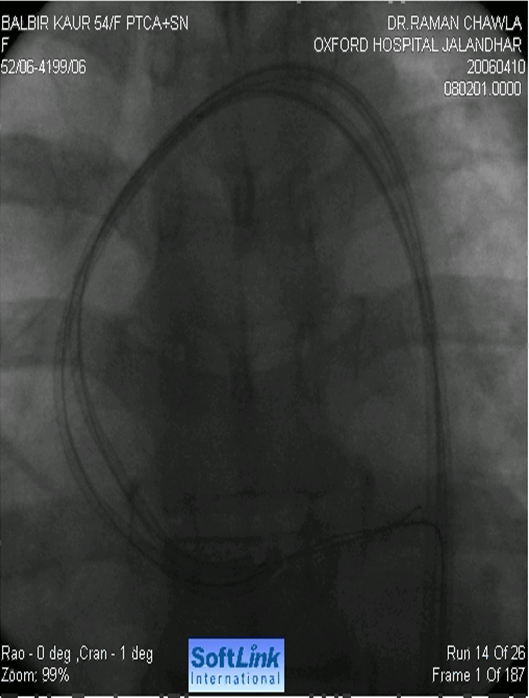
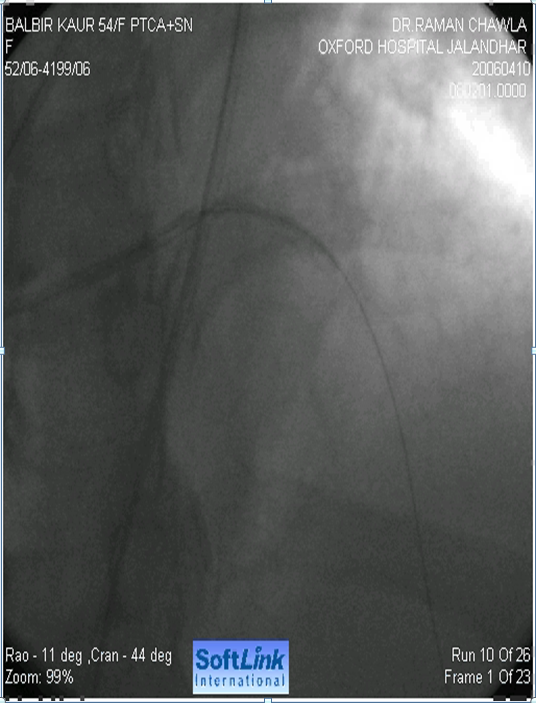
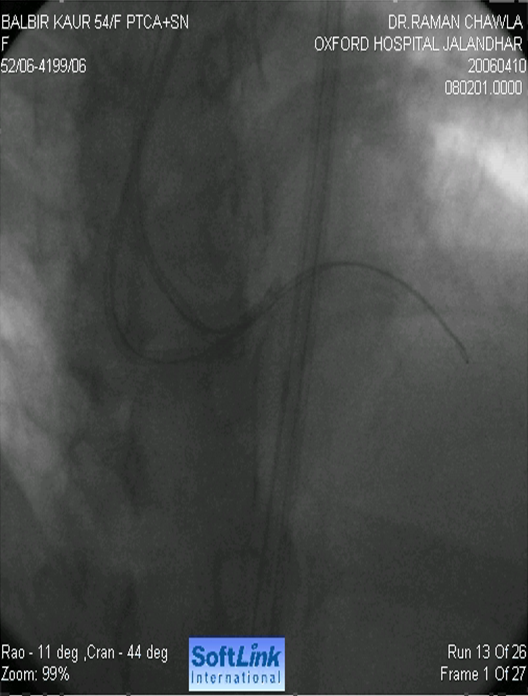
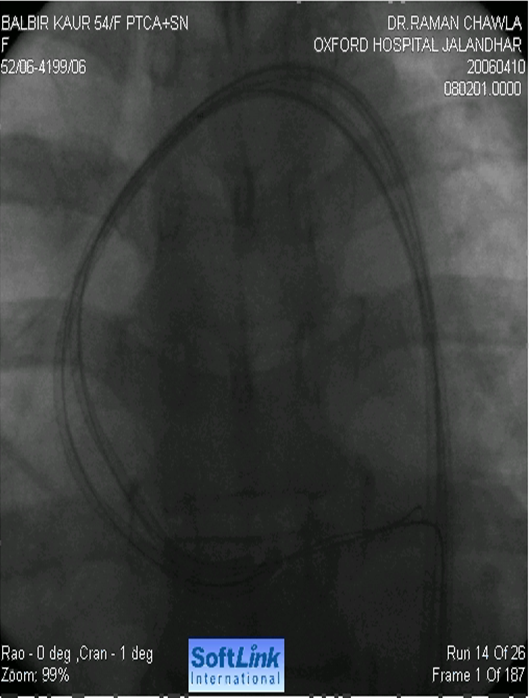
Procedural Step
Femoral approachGuiding catheter 6f jl 3.5 Guide wire 0.014 choice pt extra support. Predilated with 2.5 x 15 mm balloon. Femoral approach Guiding catheter 6f jl 3.5 Guidewire 0.014 choice pt extra support Pre dilated with 2.5 x 15 mm balloon. Attempted withdrawal Stent dislodged from balloon into left- main coronary artery. Second guide & wire fromcontralateral femoral, Stent snaired out Successful coronary angioplasty using another stent Patient discharged after three days.
Case Summary
Never withdraw the stent, Deploy there only, Carefulwithdrawal of stent in calcified vessel with proper alignment of guiding. Tryto withdraw stent, guide wire and guiding catheter as a total assembly. Snaringof stent from Left Main Coronary Artery technical expert required. Contralateral femoral puncture and simultaneous wiring if vessel goes into threaten occlusion beforeretrieval of previous wire. As previous wire will help in easy tracking down ofadditional wire. Double wire criss-cross technique. Crush the stent againstwall with another stent. Sub acute stent thrombus need aggressive management.