
CASE20220826_001
A challenging case report : contemporary LM intervention and TAVI AT THE SAME SETTING.
By ,
Presenter
TURKI AYED AL GARNI
Authors
1, 1
Affiliation
, Saudi Arabia1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
A challenging case report : contemporary LM intervention and TAVI AT THE SAME SETTING.
1, 1
, Saudi Arabia1
Clinical Information
Patient initials or Identifier Number
ATA
Relevant Clinical History and Physical Exam
A 74-year-old female known to have diabetes hypertension presentedto our clinic with shortness of breath New York Heart Association (NYHA) classIII progressively increasing for the last three months associated withorthopnea there was no history of angina or syncope. The patient has limitedfunctional capacity. She has no previous surgical history.
Relevant Test Results Prior to Catheterization
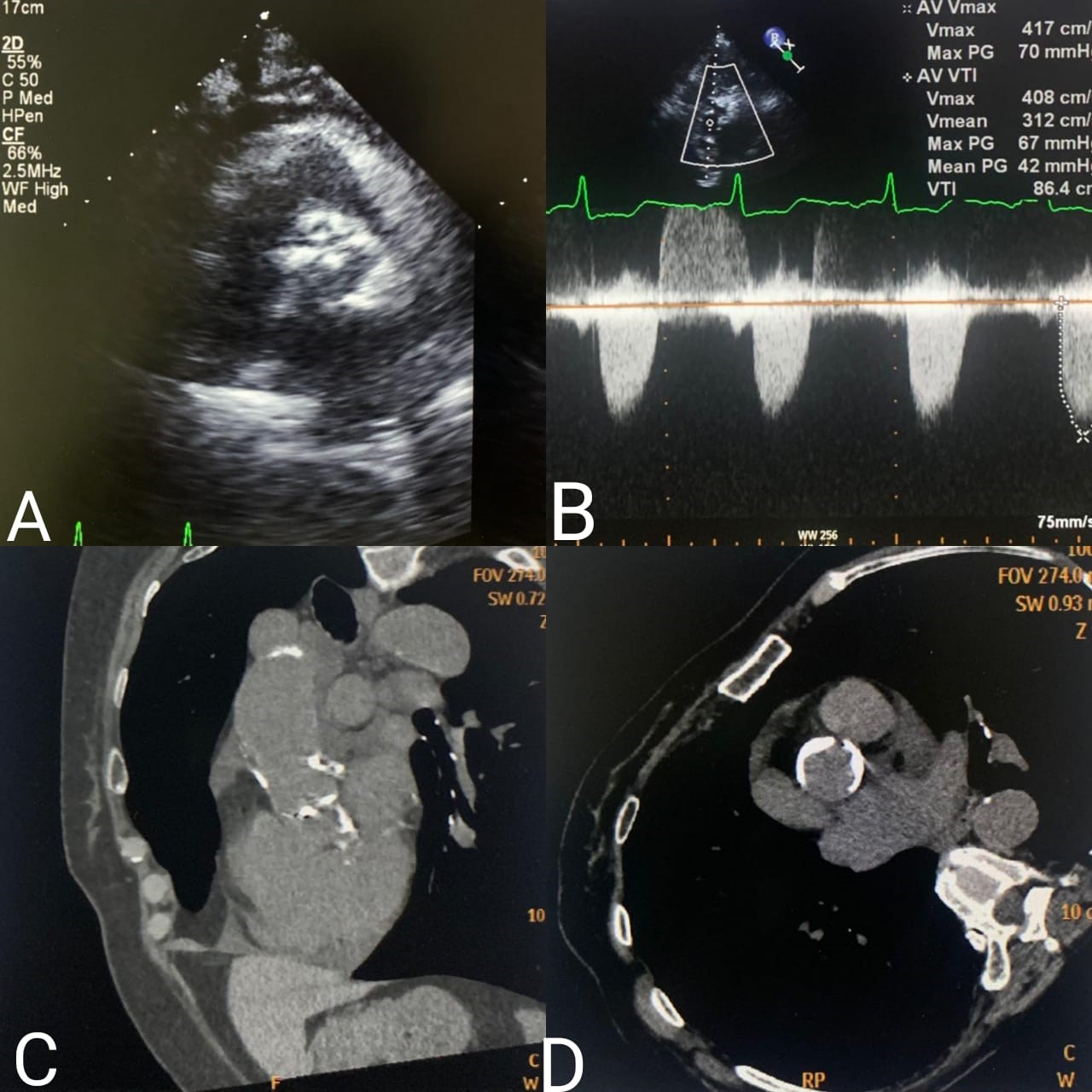
TTE revealed a left ventricular ejection fraction of 40%,hypokinesia at the mid, apical anterior septum, and apical anterior all withpreserved thickness. there was a severely thickened aortic valve with severe stenosis(FIGURE1 A&B) moderate aortic regurgitation, and severe mitral and tricuspidregurgitation. CT for calcification showed heavily calcifiedaortic root and calcification in the ascending aorta (FIGURE1 C&D). CT with contrast showed feasible measurements forTAVR
Relevant Catheterization Findings
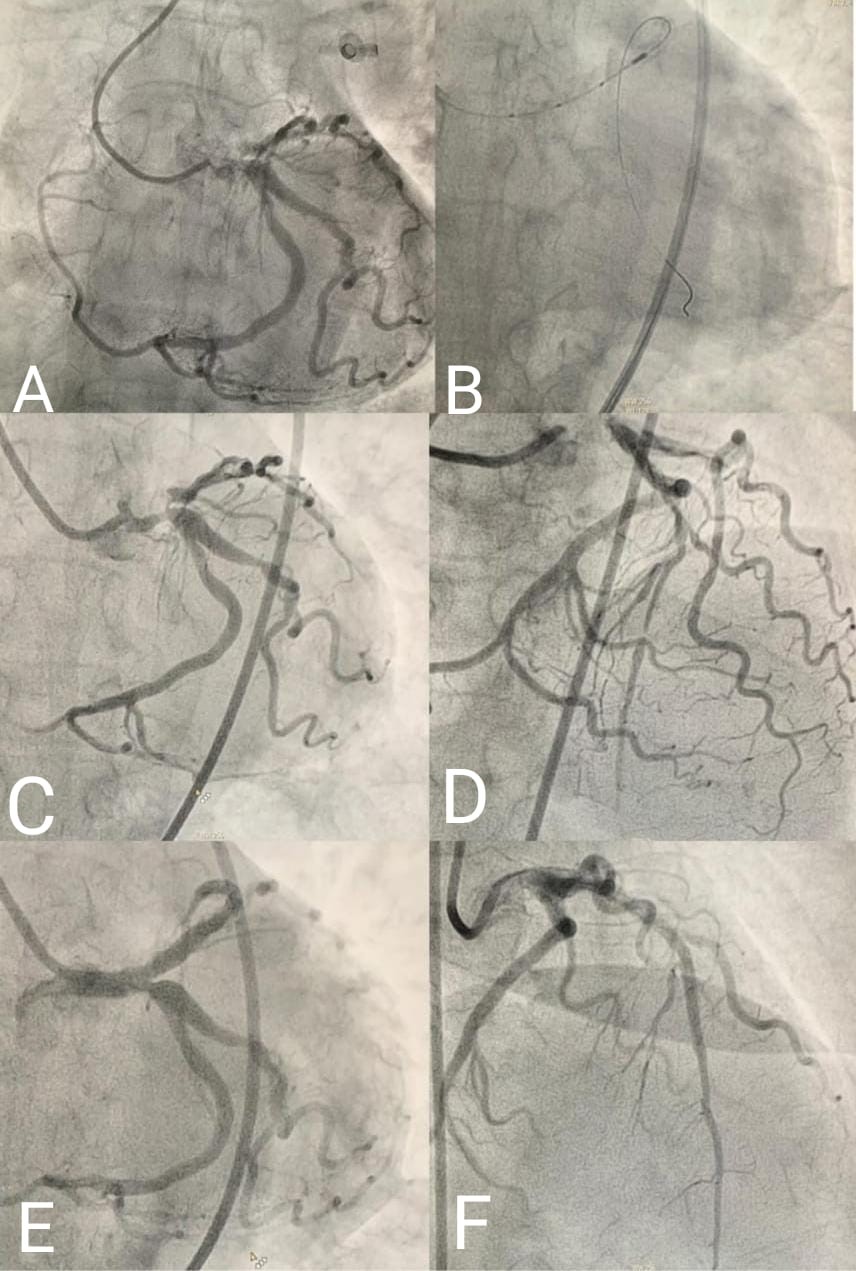
Invasive coronaryangiography showed heavily calcified LMCA with severe stenosis and heavilycalcified left anterior descending artery LAD with severe stenosis at theproximal and the mid-segment (VIDEO 01). The left circumflex artery LCX has a mild ostial disease with no significant disease distally the right coronary arteryRCA originates as a continuation of the distal LCX artery (FIGURE 2A) (VIDEO 02).
 VIDEO 01.mp4
VIDEO 01.mp4
VIDEO 02.mp4
Interventional Management
Procedural Step
The case was discussed in the MDHT. The decision was made to go for high-risk PCI and if the result isgood will proceed with TAVR in the same session under ECMO support. The patient was electively intubated then the right femoral vein and the left femoralartery were canulated for ECMO. The average support was 3.5 l/min. 7 Fr sheathto the right femoral artery and extra-backup EBU guide catheter was used toengage the LMCA. The lesion was prepared using a 2.0X15 non-compliant balloon thenintravascular ultrasound IVUS was done to LMCA/LAD, which showed 360-degree severe calcification in the midLAD all the way to the ostium and 270-degree in the LMCA then IVL using 3.0X12mm shockwave balloon to LMCA/LAD (VIDEO 03). Then two overlapping drug-elutingstents (2.75X33 mm overlapped with 3.5x38 mm) were deployed to mid LAD and thenproximal LAD to LM. Post dilated with 3.0x15 mm non-compliant balloon then 4.0x15mmnon-compliant balloon proximally and final proximal optimization techniqueusing 5.0x12 mm non-compliant balloon to the LM with good result (FIGURE2)(VIDEO 04,05). Then the transcatheter self-expandable core valve is implanted under rapidpacing (FIGURE3) (VIDEO 06,07). The patient tolerated the procedure well. theECMO was decannulated in the lab. Extubated two hours later. TTE showed EF of 60%, well seated bioprosthetic valve mildparavalvular leak moderate mitral regurgitation. The patient was discharged home after four days in a goodcondition.
VIDEO 03.mp4
VIDEO 04.mp4
VIDEO 05.mp4
VIDEO 06.mp4
VIDEO 07.mp4
Case Summary
Our case showed the importance of choosing theappropriate mechanical circulatory support system in different case scenarios. Thefull hemodynamic support gives the operator the chance to optimize the resultof the high-risk intervention. Future randomized trials may help to guidechoosing the modality of mechanical circulatory support. The heavily calcifiedcoronary lesions need good lesion preparation for a better outcome.