
CASE20220819_001
Tip In Technique as bailout in a Retrograde CTO PCI in Philippine Heart Center: A case report
By , ,
Presenter
Anna Katrina Ng Chua
Authors
1, 1, 1
Affiliation
, Philippines1
Complex PCI - Chronic Total Occlusion
Tip In Technique as bailout in a Retrograde CTO PCI in Philippine Heart Center: A case report
1, 1, 1
, Philippines1
Clinical Information
Patient initials or Identifier Number
ADC
Relevant Clinical History and Physical Exam
A 61 year old male ,hypertensive,diabetic , non compliant to medications, with history of stroke with left sided residuals, 50 pack year smoker and previous heavy alcoholic drinker .He presented with severe, substernal chestpain 8 hours prior to admission accompanied by shortness of breath and diaphoresis. Managed as a case of STEMI of Inferior wall, in Cardiogenic Shock, with Ventricular tachycardia.Synchronized Cardioversion and ACLS was done an patient was transferred in PCI capable institution.
Relevant Test Results Prior to Catheterization
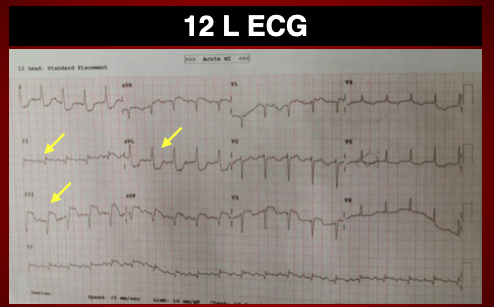
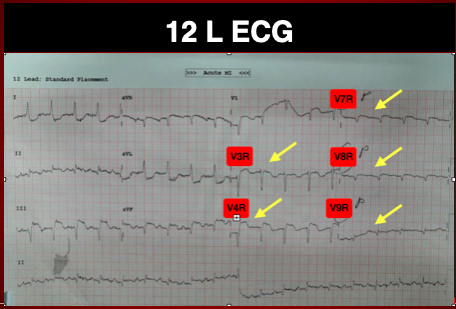
12 L ECG ST elevation leads II, III, aVF ( inferior wall) V3R V4R ( RV extension) and V7 , V8 ( Posterior wall)
Relevant Catheterization Findings
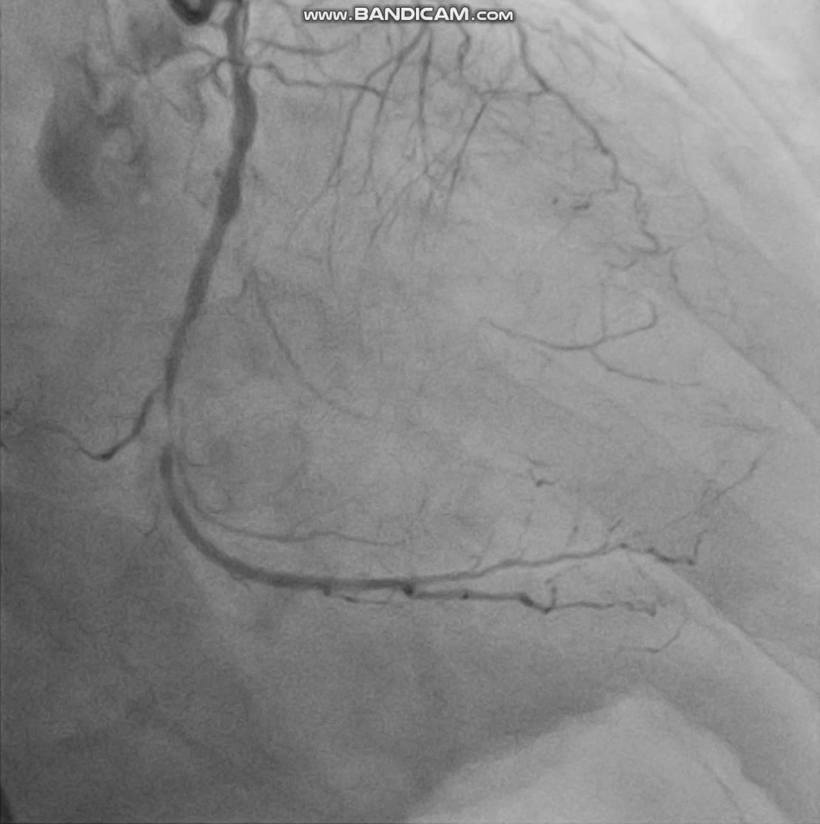
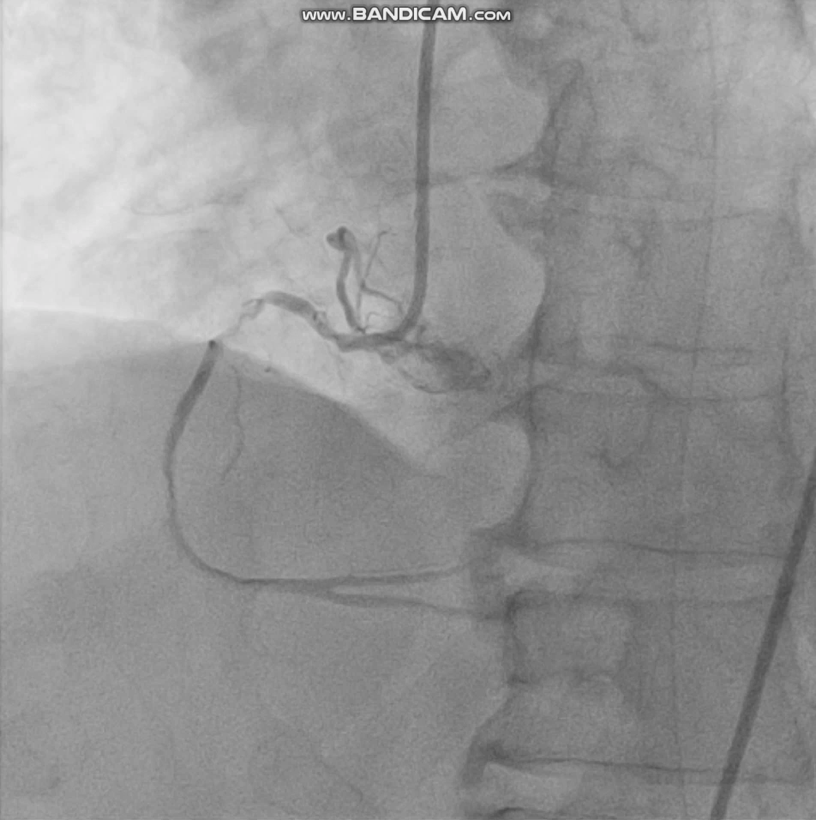
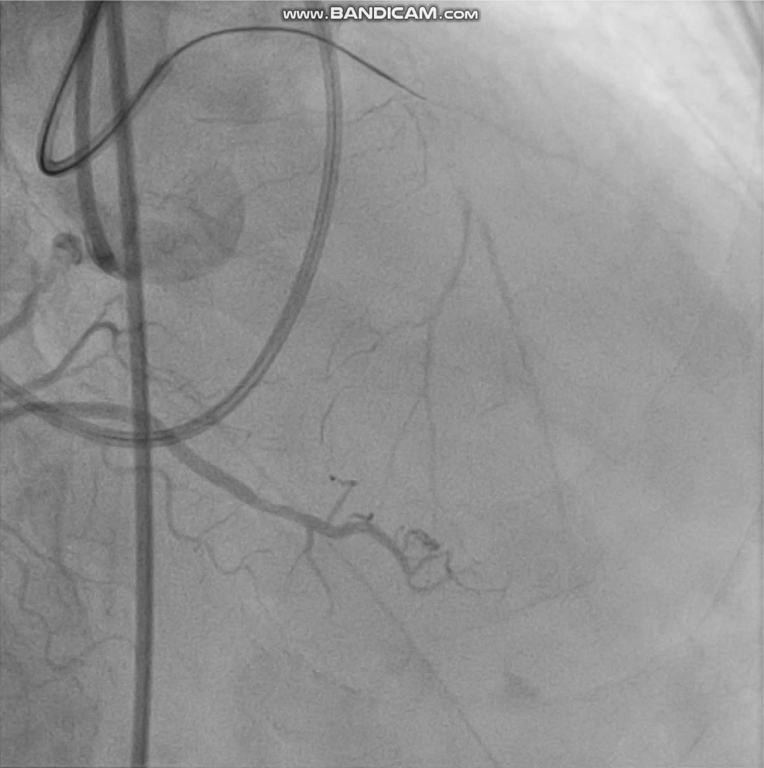
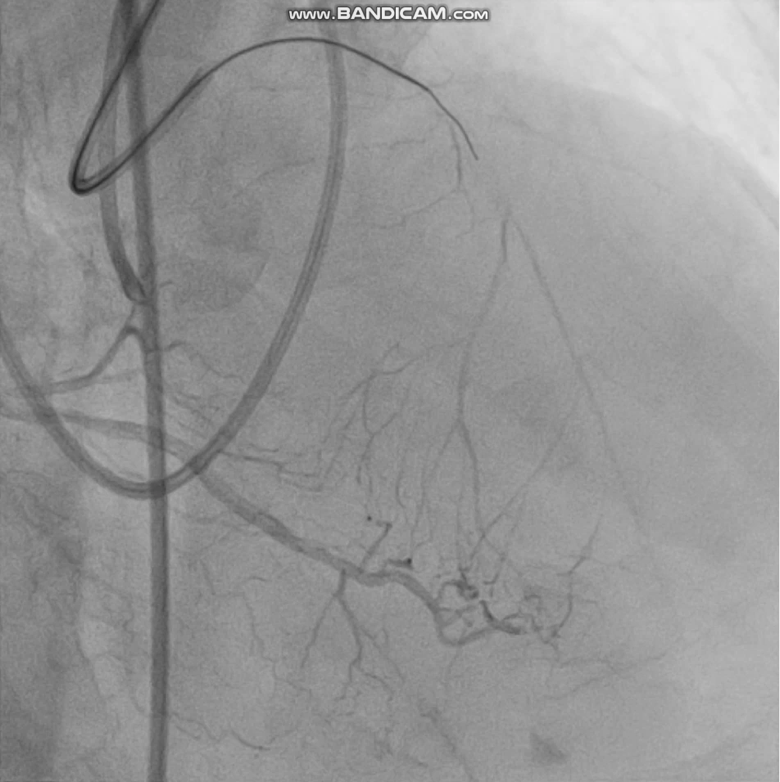
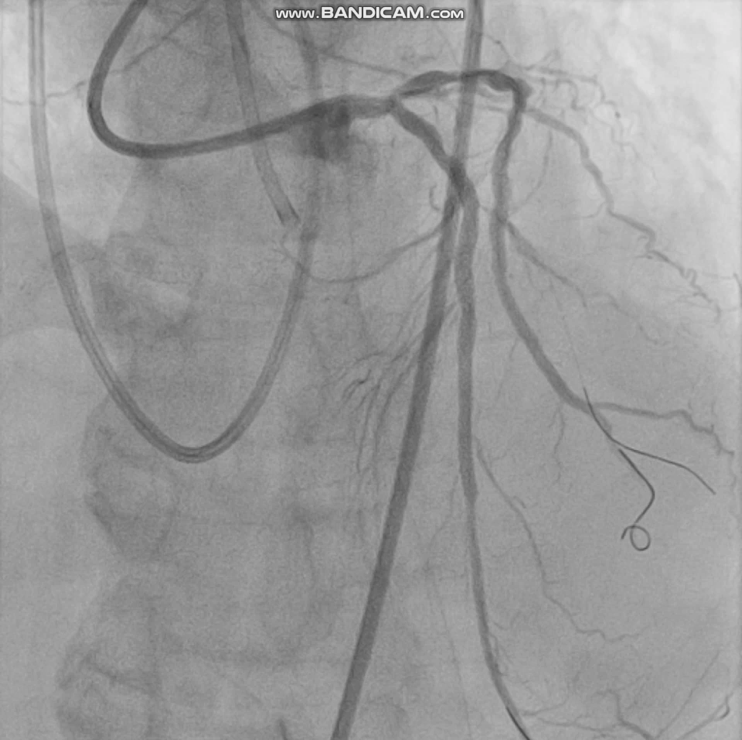
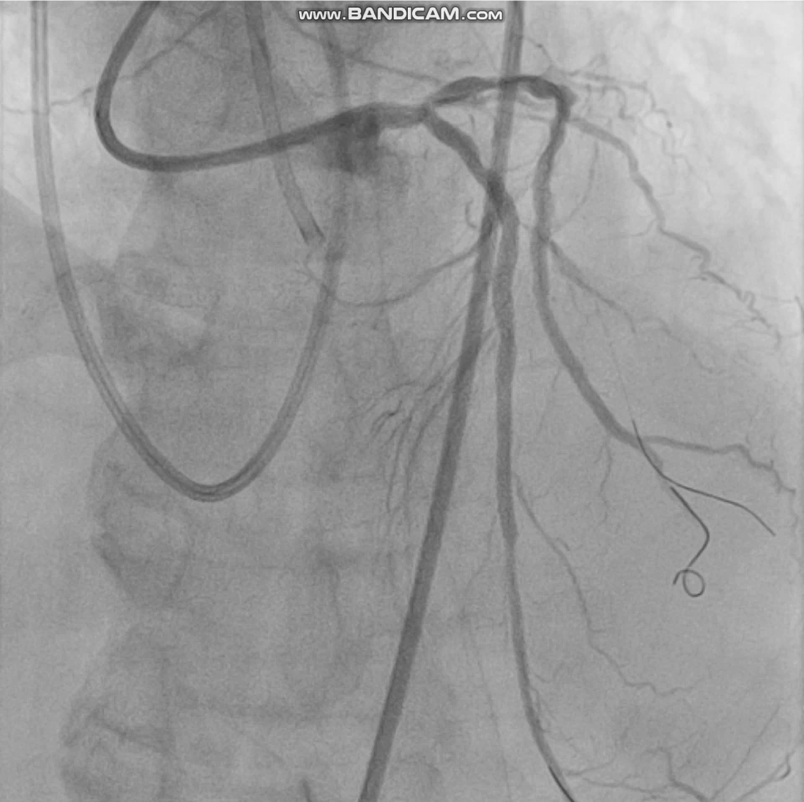
Left main has 50% distal segment stenosis. LAD had 95% ostioproximal segment stenosis becoming totally occluded at the proximal segment before D1 , the more distal segment is visualized via right to left collaterals. LCx, non dominant with 70-80% mid segment stenosis and 95% distal segment stenosis. RCA dominant with 70% aortoostial segment stenosis associated with ventricularization of pressure followed by 99% proximal segment stenosis


Interventional Management
Procedural Step
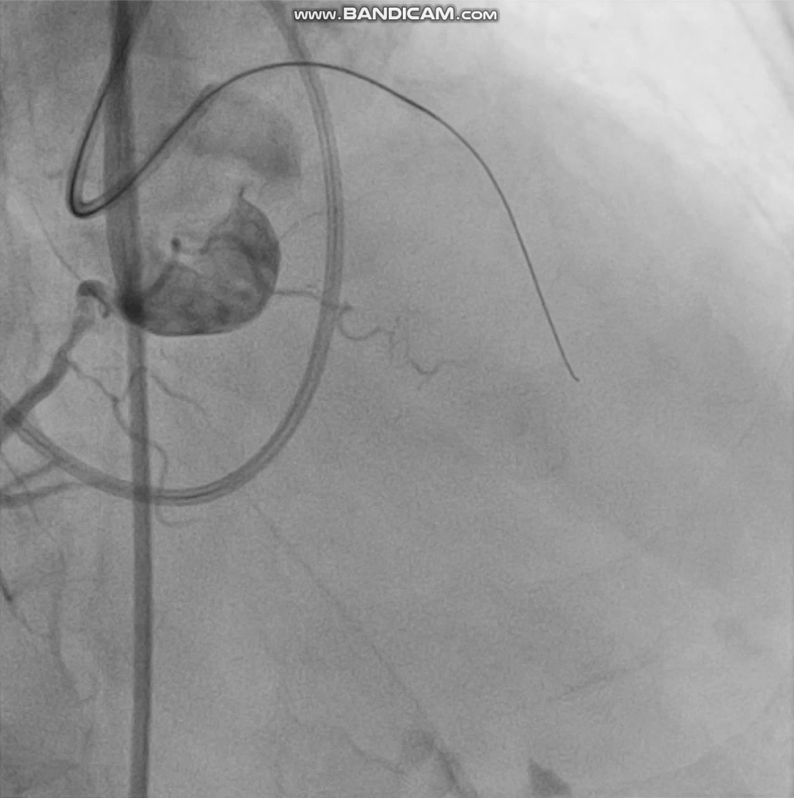
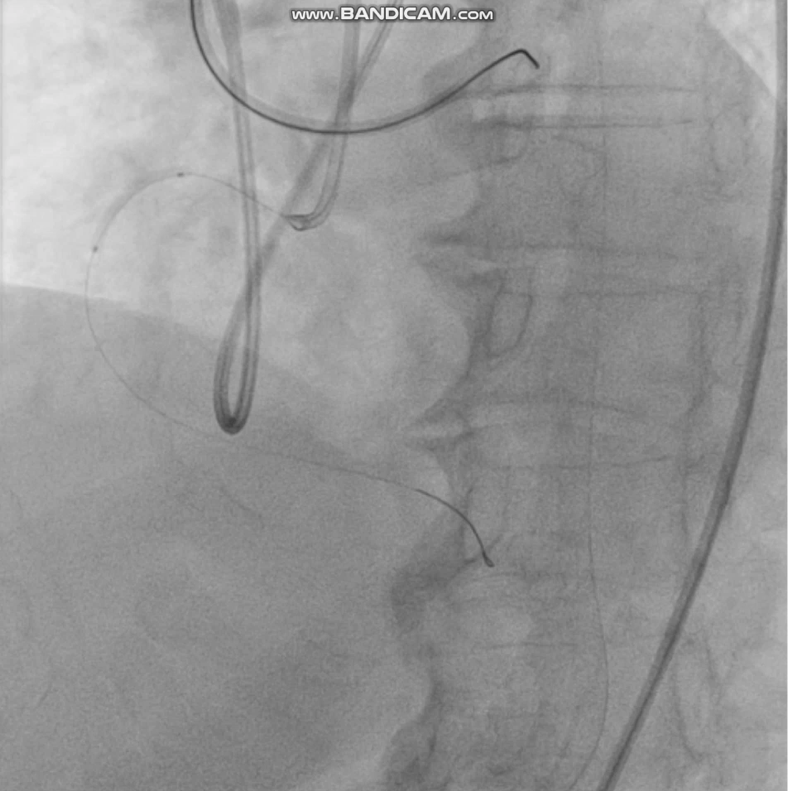
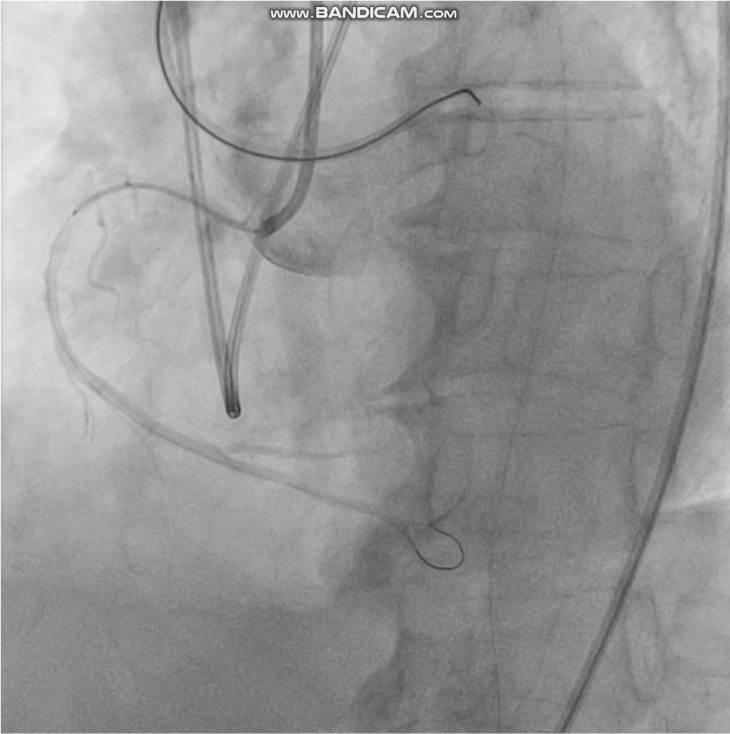
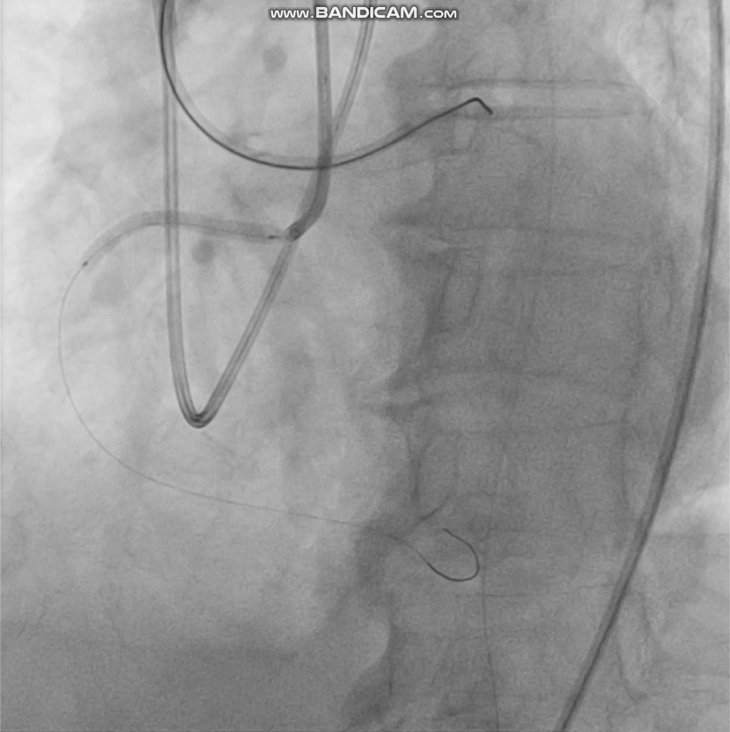
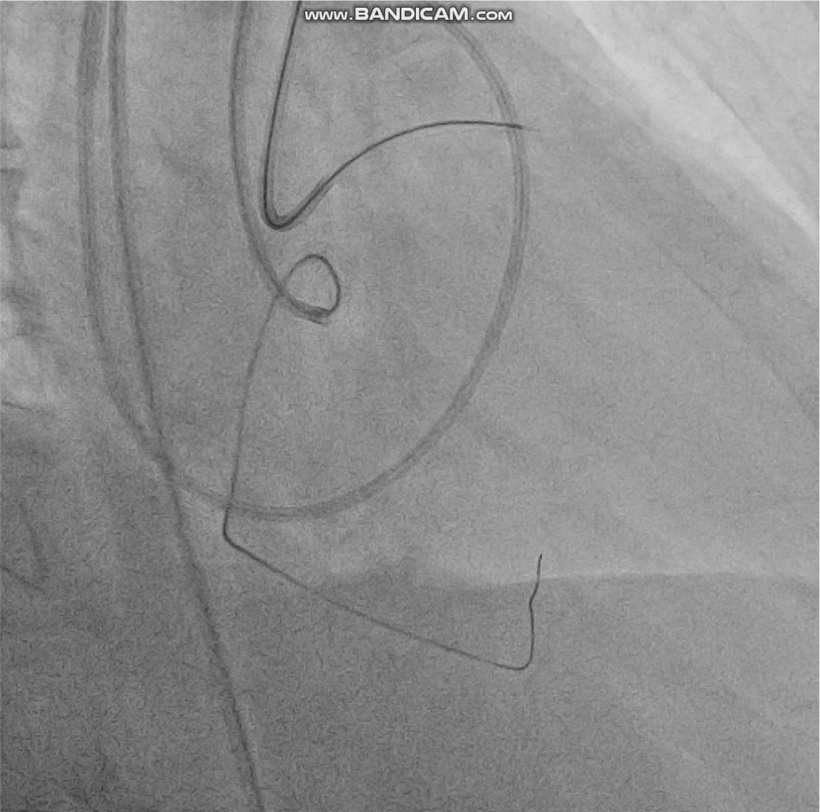
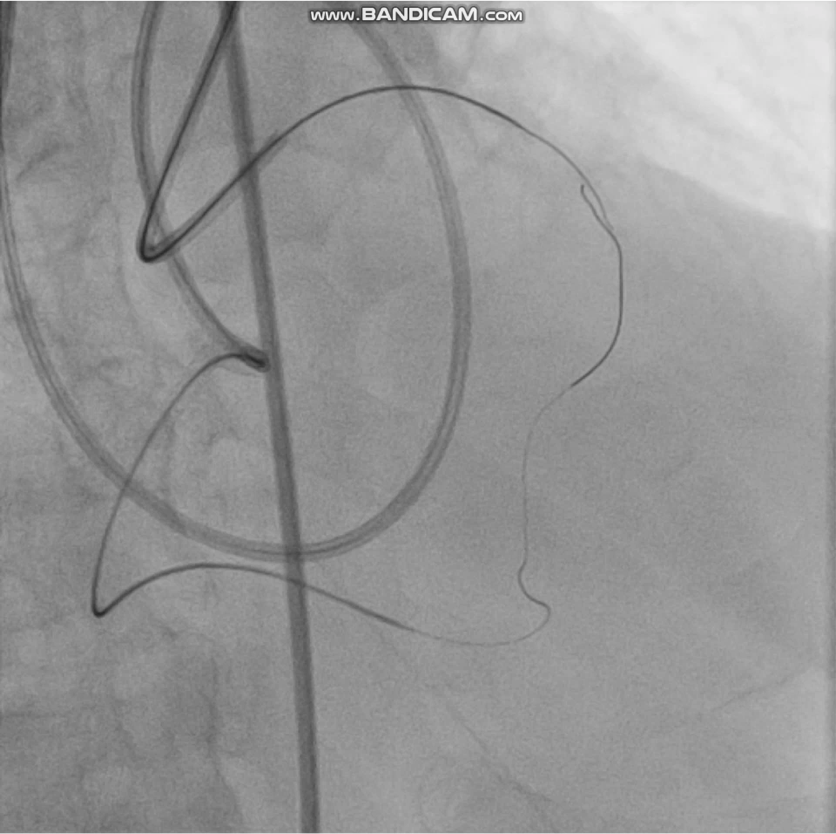
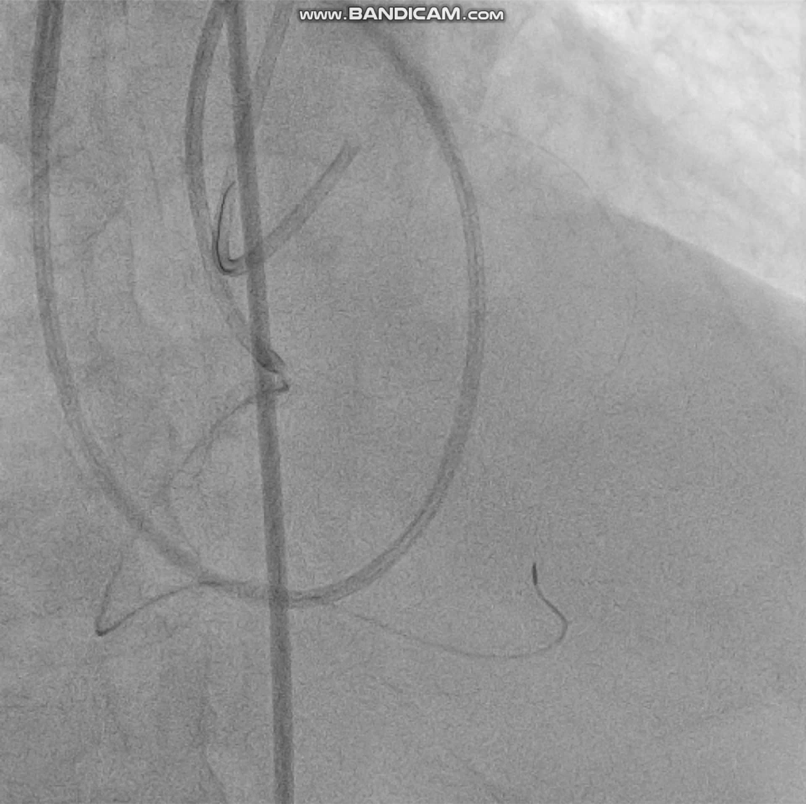
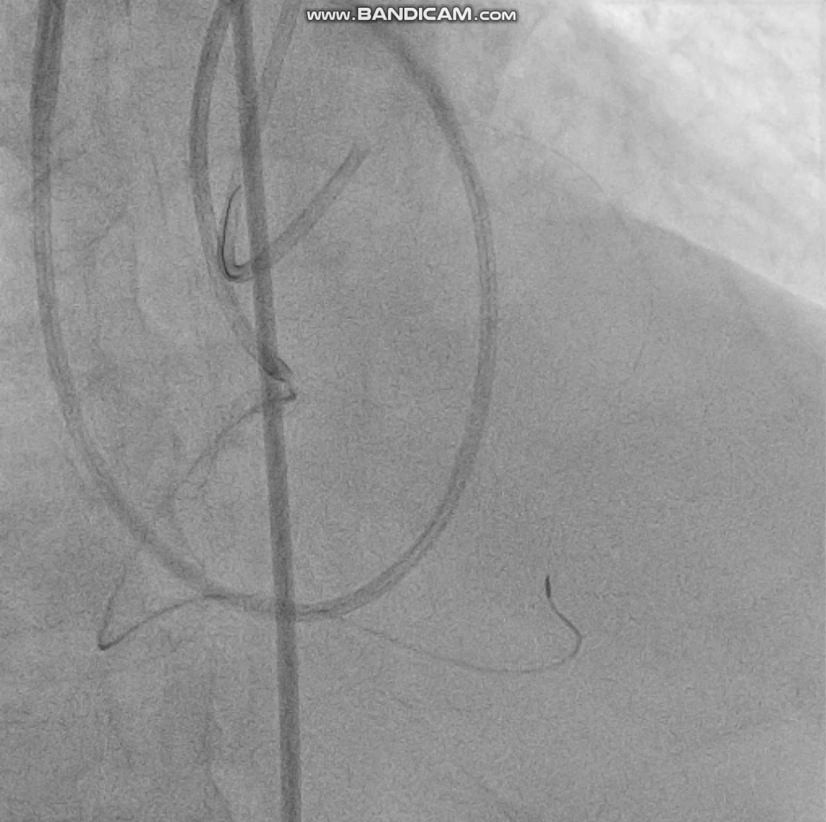
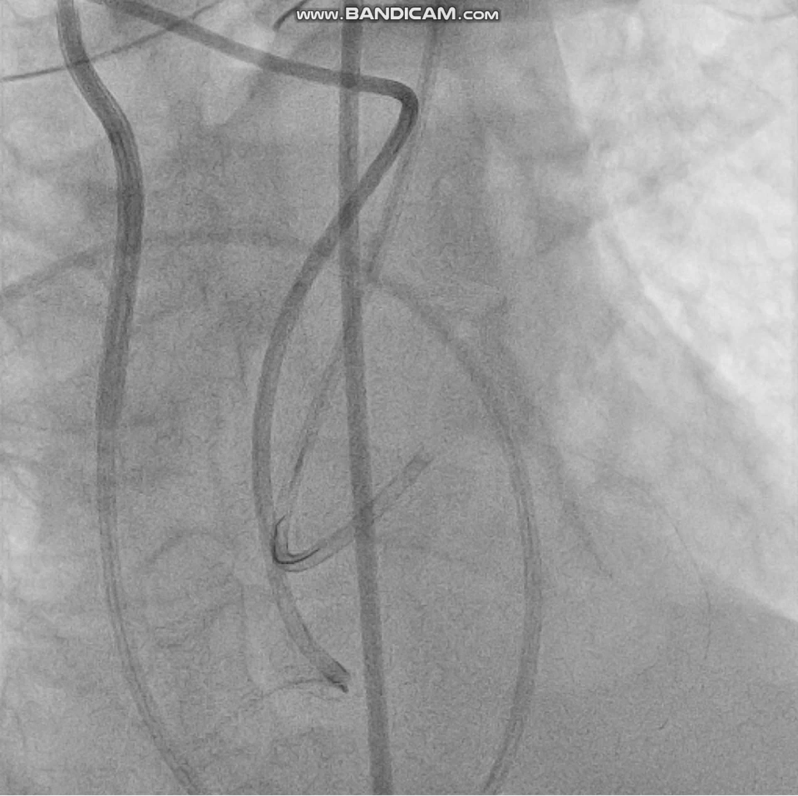
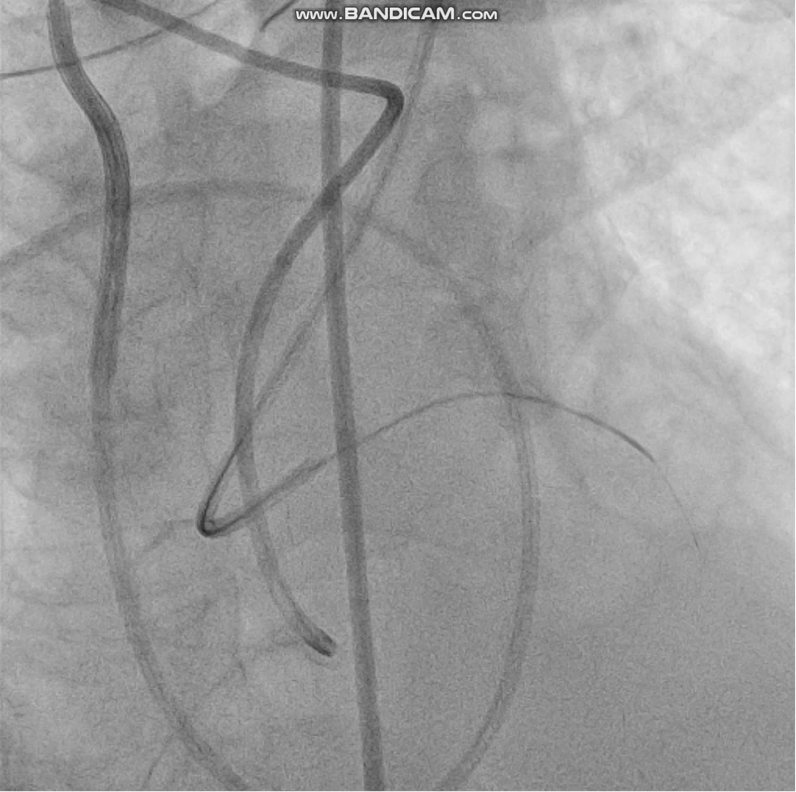
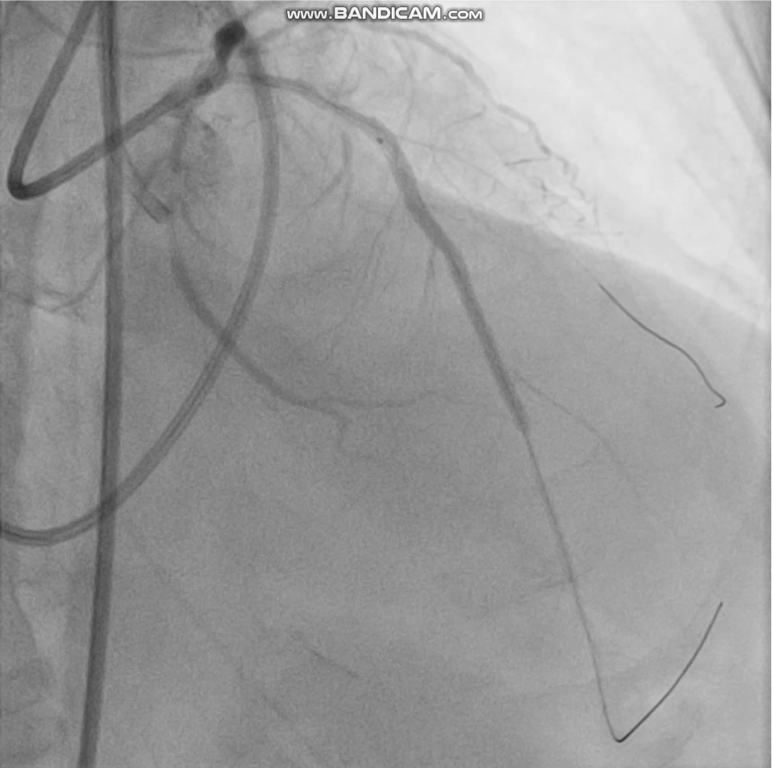
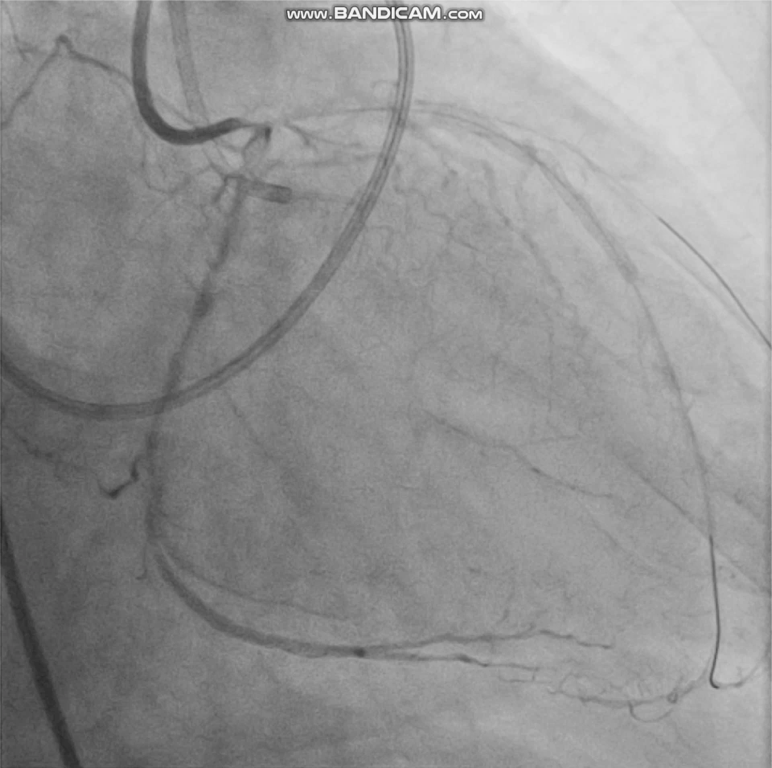
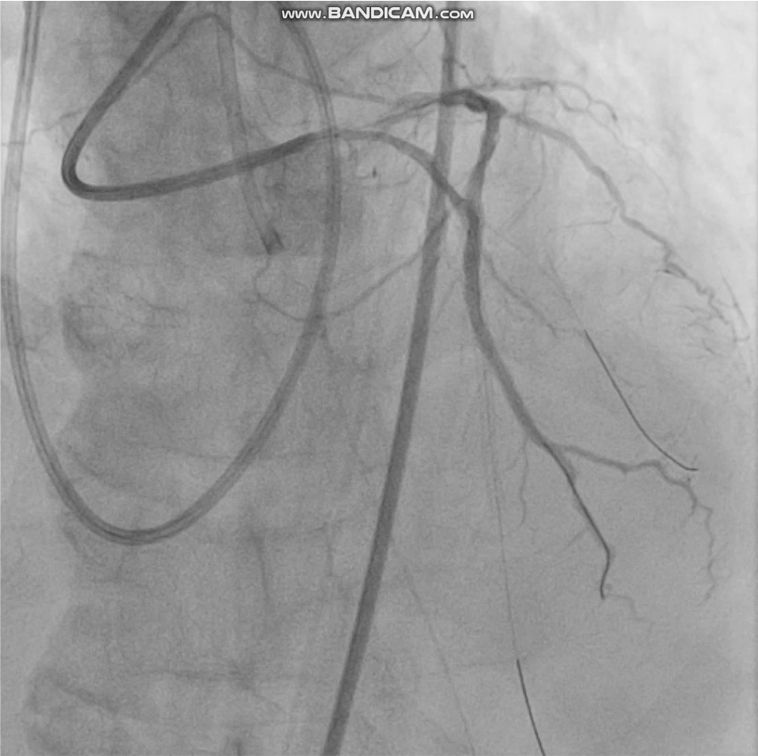
POBA of RCA was done in the index event with result of TIMI 3 flow. IABP was inserted with LVEDP of 52mmHg. Plan initially is to send patient for CABG but Heart team approach computed high STS and Euroscore, hence referred back for multivssel complex PCI. Antegrade wire escalation using Corsair Pro Asahi Microcatheter initially loaded with Sion Blue until it reaches the CTO proximal cap. Wire exchange done with Asahi Fielder XT-A with and later on exchanged with a Gaia 3rd Asahi within the microcatheter but went into the subintimal space confirmed by donor vessel injection several times Plan is to go retrograde approach but we proceeded with PCI of the proximal RCA 1st and deployed a a 3.0 x 32mm DES in the aortoostial to the proximal segment of the RCA.Septal surfing using a Caravel Asahi Microcatheter loaded with Asahi sion blue and was exchanged with Asahi Suoh 3 and finally Asahi Sion which successfully crossed the 2nd septal collateral and was positioned at the tip of the distal cap of CTO.Retrograde wire escalation using a Gaia 3rd Asahi exchanged to a Asahi Conquest Pro 12 used to do retrograde true lumen puncture. Retrograde microcatheter attempted several times but with resistance. Tip in technique was done by advancing the antegrade microcatheter over the retrograde guidewire in the antegrade guide. Double lumen microcatheter was inserted in place of antegrate micro catheter which facilitated wiring of mid to distal LAD. PCI proceeded antegradely with DES.






Case Summary
Tip in technique is done by advancing the antegrade microcatheter over the retrograde guidewire in the antegrade guide, allowing easy, predictable, and successful antegrade wiring by inserting a wire into the antegrade microcatheter which allows successful revascularization of a CTO after failure to externalize. Advantages include decreased risk of vessel injury, decreased risk of donor vessel ischemia, decreased risk of bleeding and decreased risk for wire entrapment .