
CASE20220818_006
An Interesting Case: Single Vessel but a Calcified CTO With Stenting Across the Left Main.
By , , , , , , , ,
Presenter
Benjamin Tao Xiung Lim
Authors
1, 1, 1, 1, 1, 1, 1, 1, 1
Affiliation
, Malaysia1
Complex PCI - Calcified Lesion
An Interesting Case: Single Vessel but a Calcified CTO With Stenting Across the Left Main.
1, 1, 1, 1, 1, 1, 1, 1, 1
, Malaysia1
Clinical Information
Patient initials or Identifier Number
HBH
Relevant Clinical History and Physical Exam
Mr HBH is a 68 year old gentleman, active smoker of 35 pack years, with hypertension and dyslipidemia. He was referred from a district hospital due to admission in August 2020. He presented with typical chest pain and diaphoresis, then was treated for a NSTEMI.
 20220726_131910.mp4
20220726_131910.mp4
20220726_132034.mp4
20220726_132441.mp4
Relevant Test Results Prior to Catheterization
ECG done showed sinus rhythm with T wave in version over anteriorleads. Troponin I was 3.54. Echocardiography in October 2020, showed anejection fraction of 60%, no regional wall motion abnormalities with trivialaortic regurgitation. His renal function was normal with a creatinine of 80umol/L.
20220726_132727.mp4
20220726_133046.mp4
Relevant Catheterization Findings
Coronary angiography done in May 2022 showed single vessel diseasewith a short LMS, calcified LAD with ostial LAD CTO and collaterals from RCA,LCx was smooth, RCA was dominant with mid segment RCA having 30 – 40% stenosis.He was subsequently planned for a stage PCI to CTO LAD in July 2022.
20220726_133721.mp4
20220726_134055.mp4
20220726_134303.mp4
Interventional Management
Procedural Step
Bilateral puncture with 6Fr sheath for right radial access and 7Fr sheath for right femoral access.
20220726_134516.mp4
20220726_134538.mp4
Case Summary
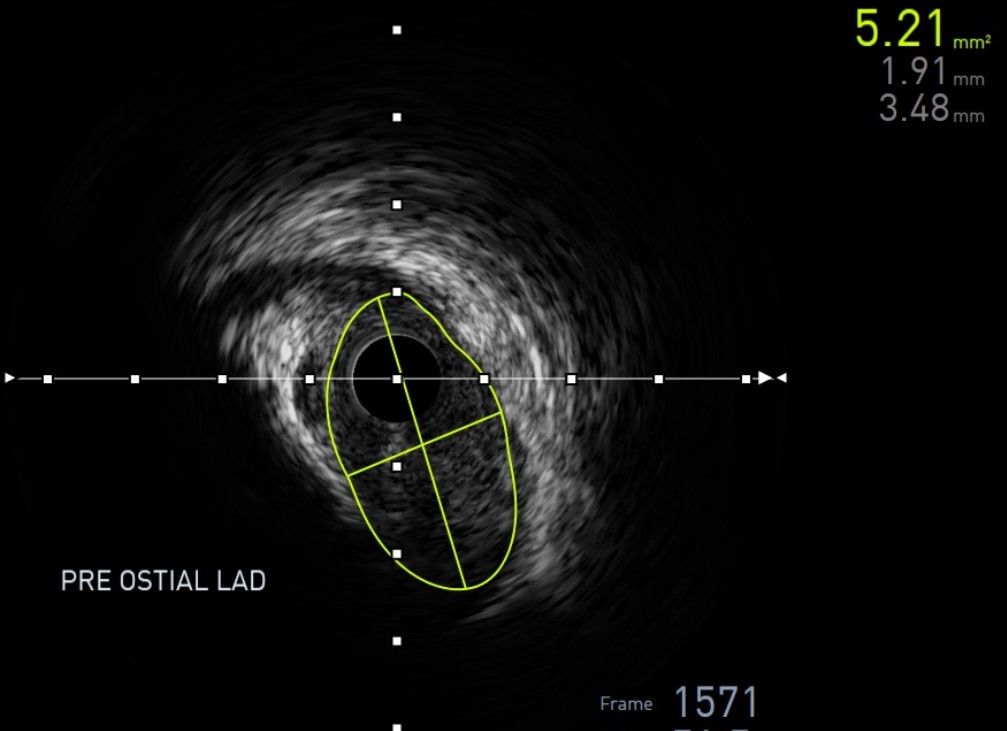
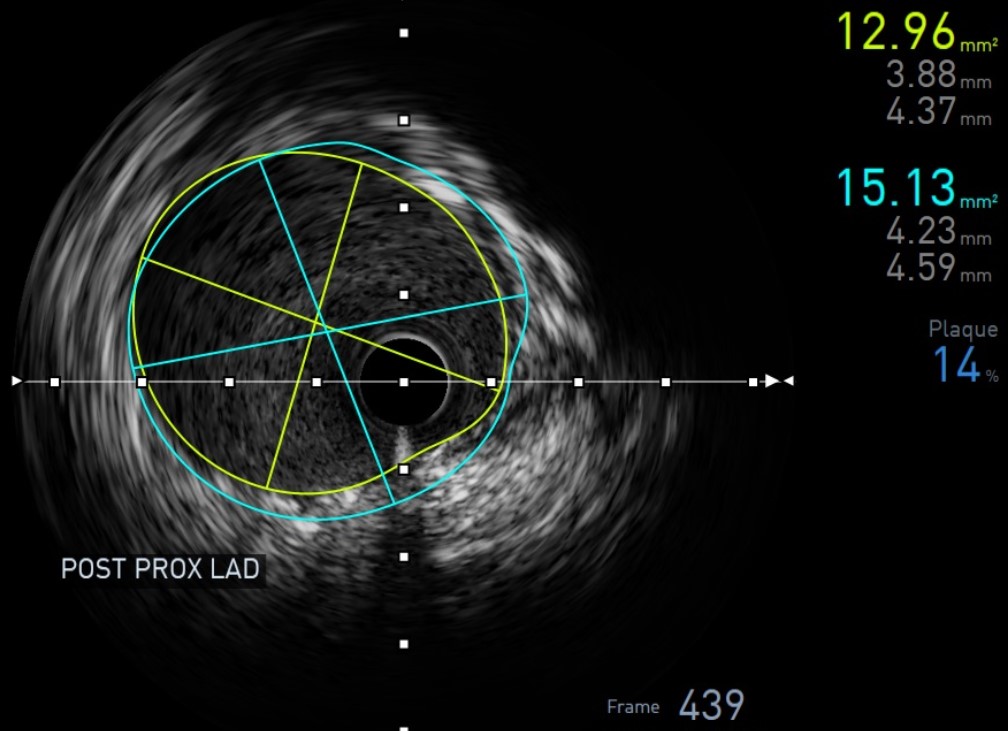
IVUS run post, no stent edge dissection, well opposed and well expanded. Distal LAD MLA 5.78 mm2, mid LAD MLA 8.10 mm2, proximal LAD MLA 12.96mm2. Stent covered till ostial LM and LM - LAD MLA was 12.28 mm2.