
CASE20220818_003
Retrograde recanalization of CTO of the RCA
By , , , ,
Presenter
Pavel Emelyanov
Authors
1, 1, 1, 1, 1
Affiliation
, Russian Federation1
Complex PCI - Chronic Total Occlusion
Retrograde recanalization of CTO of the RCA
1, 1, 1, 1, 1
, Russian Federation1
Clinical Information
Patient initials or Identifier Number
Gushin Ivan Andreevich
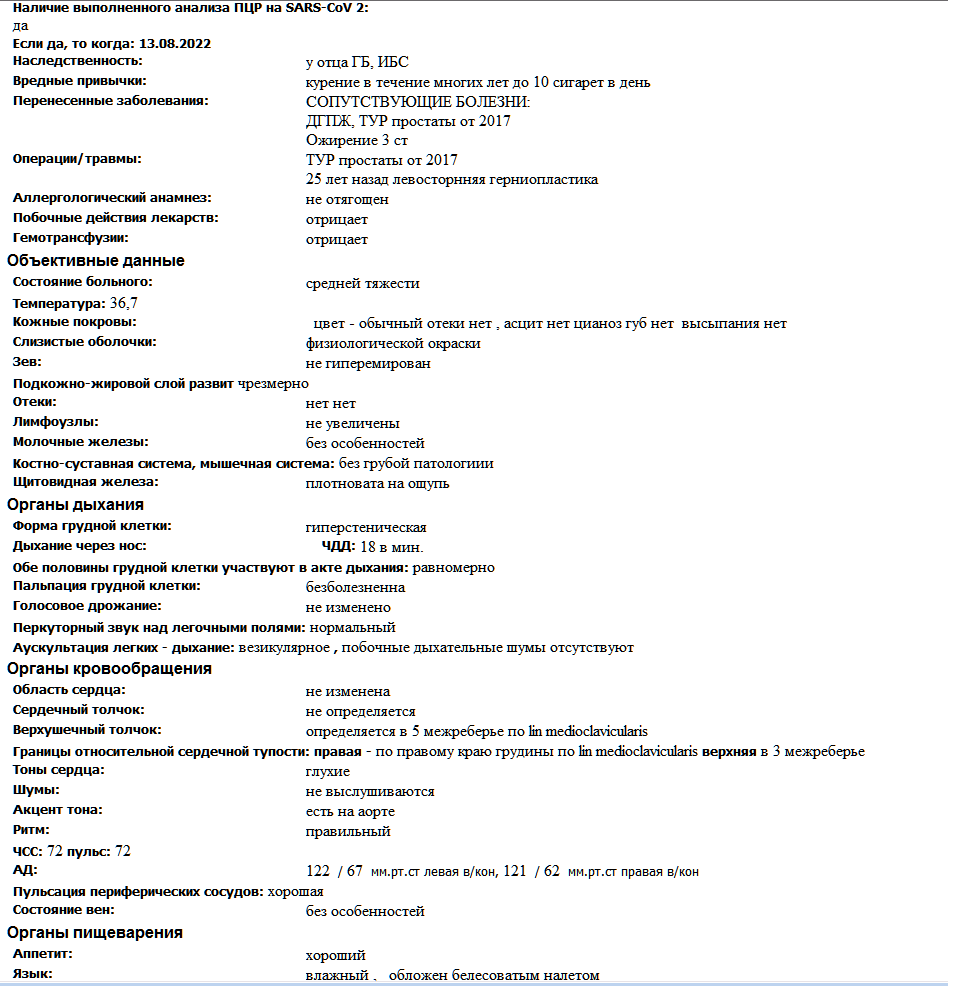
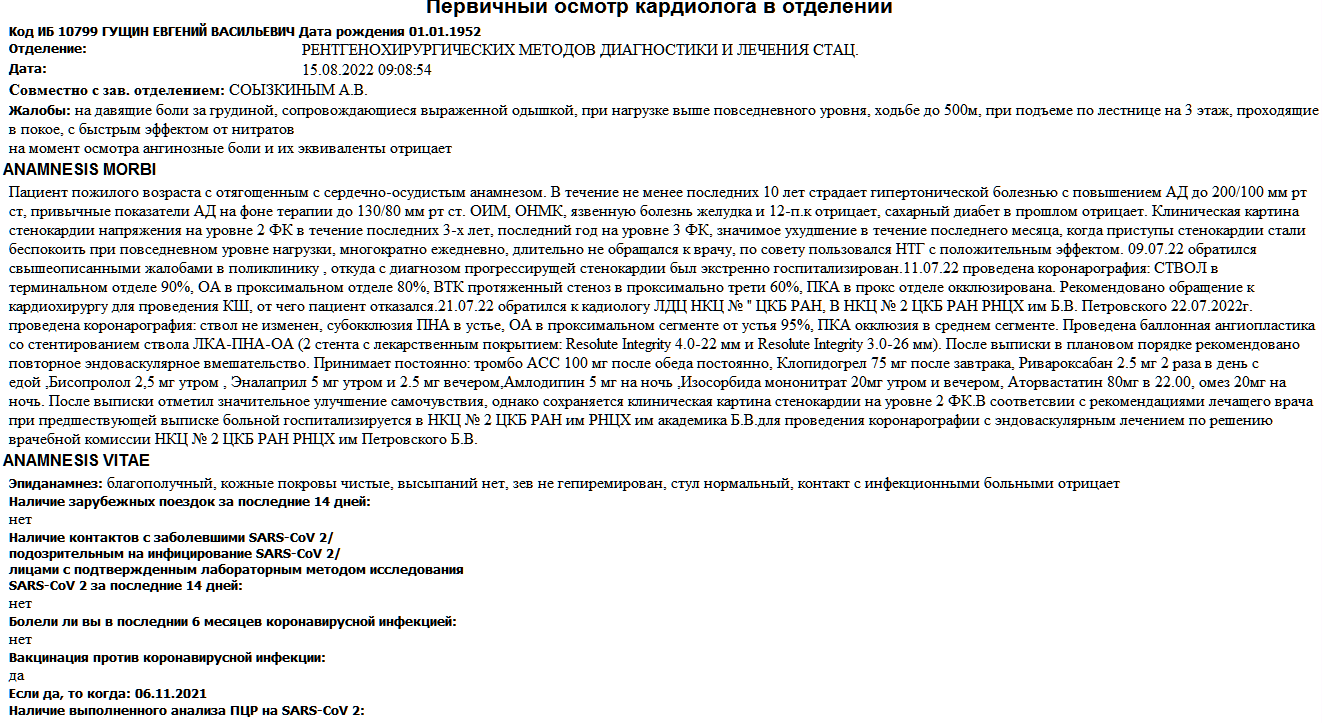
Relevant Clinical History and Physical Exam
A61-year-old patient was admitted with a diagnosis of coronary artery disease,angina pectoris, FC 3, HD III Anamnesis: considers himself ill since January2022. When I first began to notice the appearance of compressive, pressing painbehind the sternum.
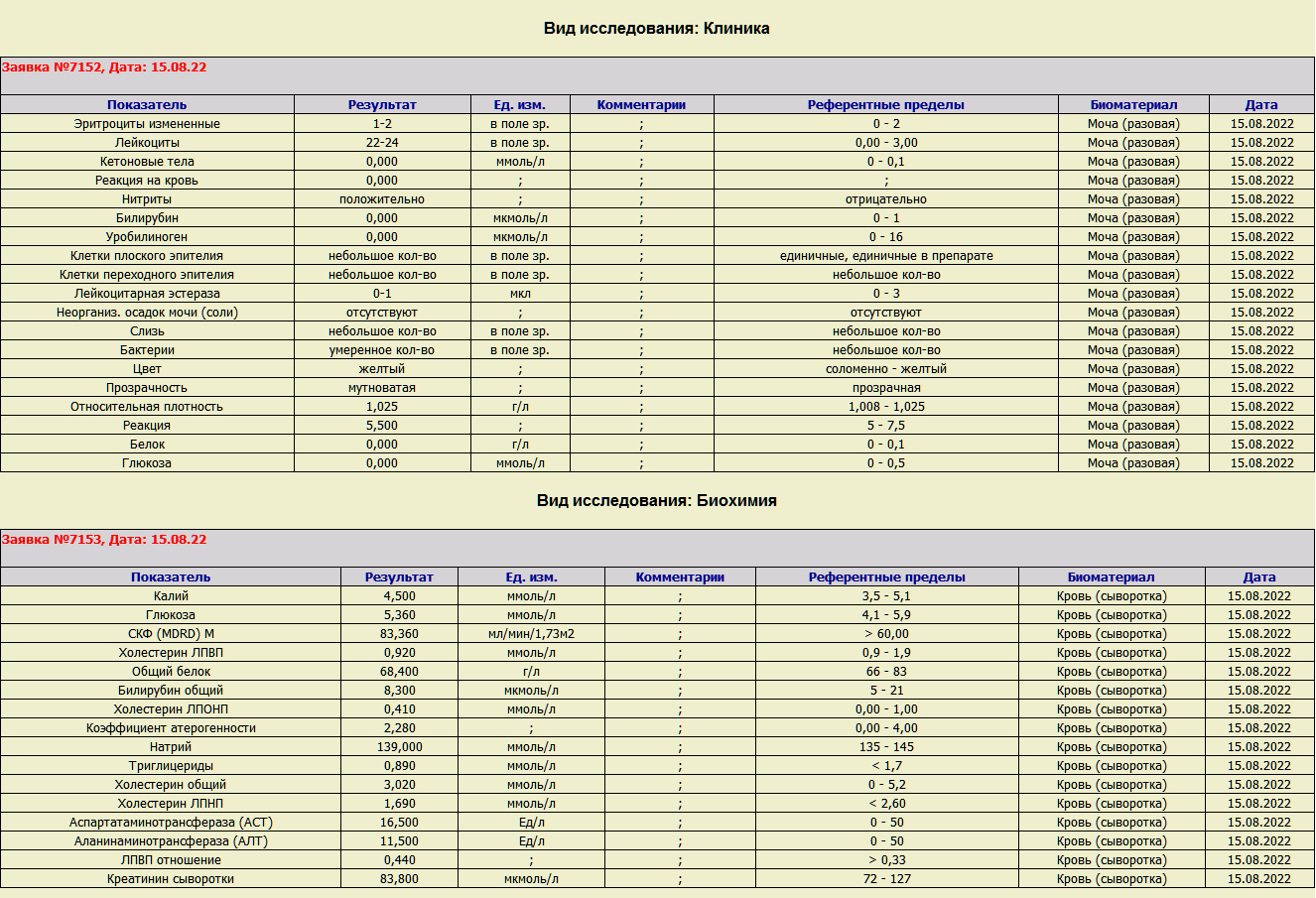
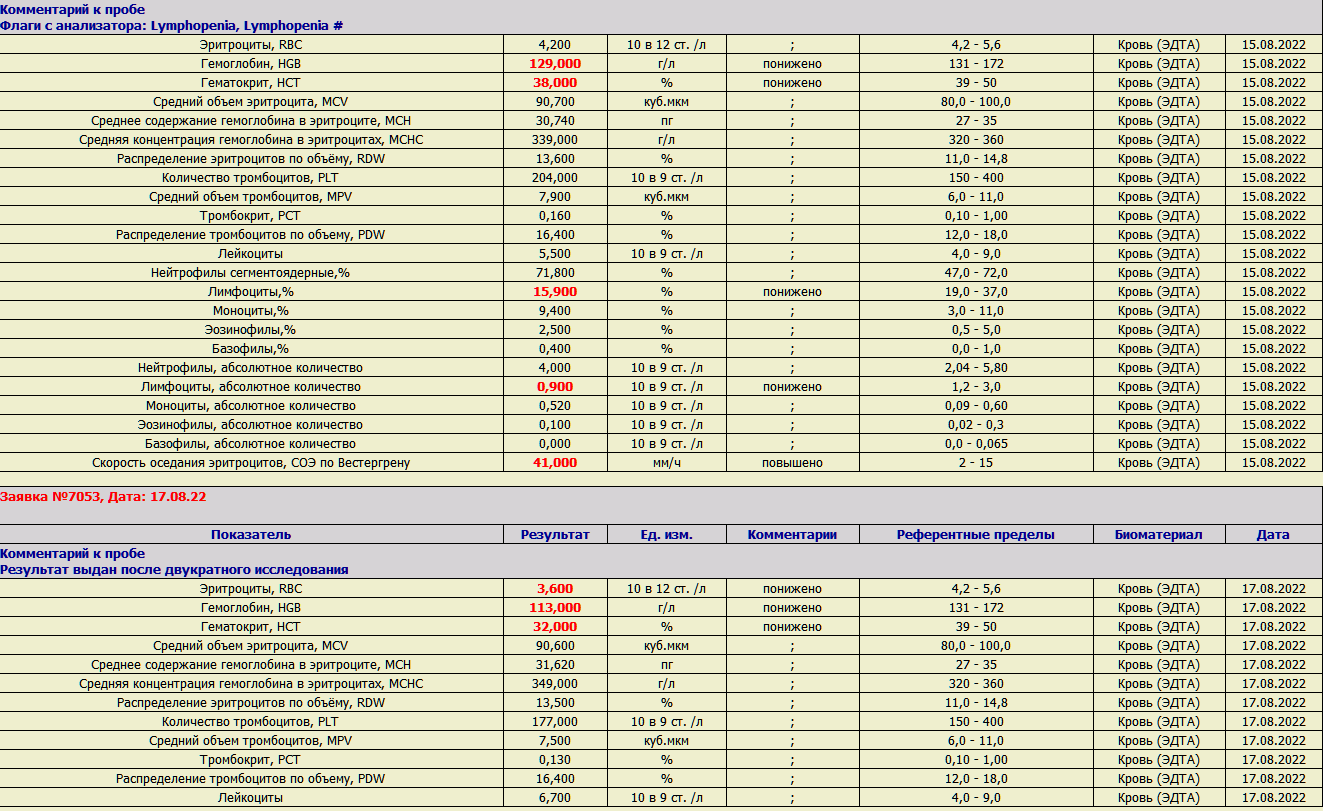
Relevant Test Results Prior to Catheterization
Rbc – 4.2(N 4.2-5.6) Hgb – 113 g/l (N 131-172), HCT– 38 (N 39-50), MCV – 90 (N 80-100), MCH-30 (N 27-35), MCHC – 339 (N 320-360), PLT – 204 (N 150-400), MPV 7.9 (N 6-11), Lei – 5,5 (N 4-9), RDW – 13.6 (N 11-14.8)
Relevant Catheterization Findings
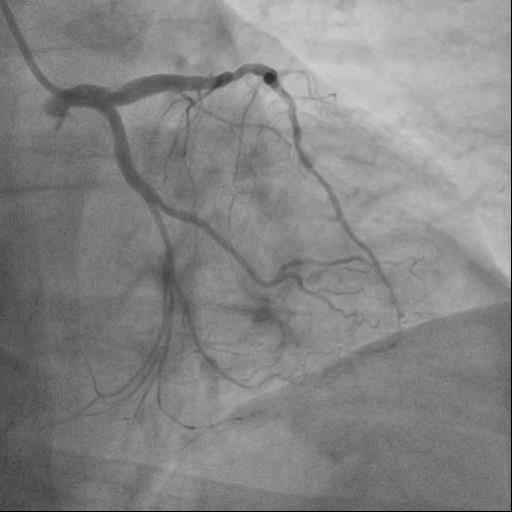
Performed coronary angiography according to the following data: LCA trunk throughoutthe stented area. LAD and LCX in the proximal segments were further stented with uneven contours. Calcification CTO of the RCA
Interventional Management
Procedural Step
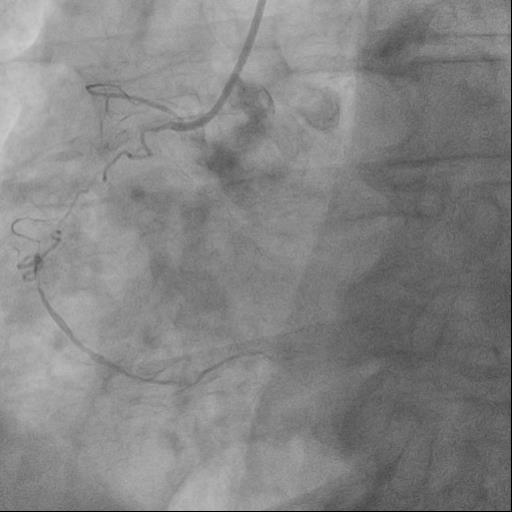
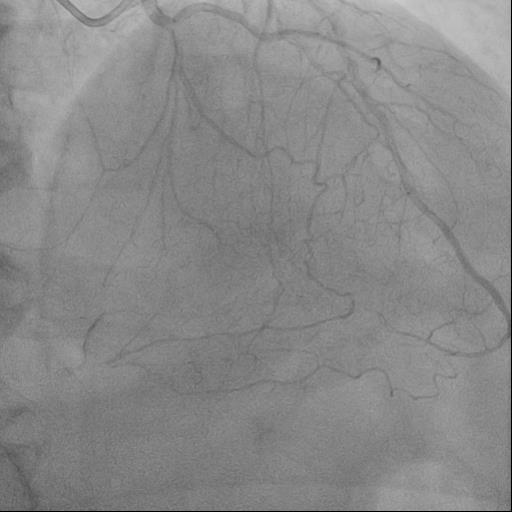
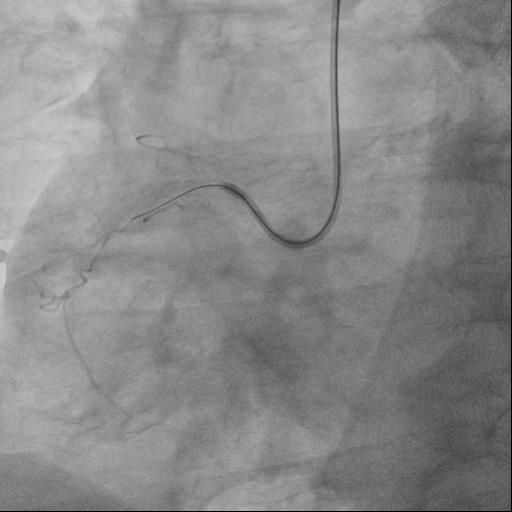
AL1 was placed at the ostium of the RCA, with the support of a microcatheter Corsair, the proximal operculum of the calcified ASB was successfully penetrated. Further, it was decided toperform retrograde recanalization of the RCA. Through the first septal branch,it was possible to bring the wire into the distal segment of the RCA. Escalated to the Gaia second wire and successfully penetrated the distal ASB cover. Further, extranalization was successfully performed using the Reverce CART technique, followed by predilation and implantation of 4 DES.
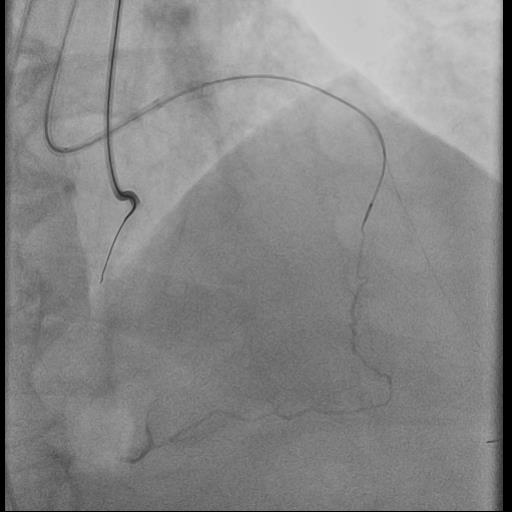
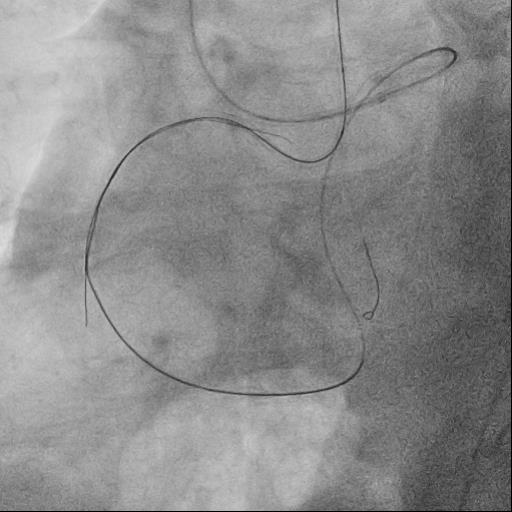
 REVERSE CART 11 .avi
REVERSE CART 11 .avi
STEP 4.avi
STEP 5.avi
Case Summary
It is very important to estimate the complexity of CTO in advance, it isdesirable to evaluate CTO on several scales, since in this case the collateralnetwork is well developed, the PROGRESS CTO - SCORE scale was applied, whichincludes predictors of the hybrid CTO recanalization approach. Retrograde CTOrecanalization minimizes the risks of antegrade wires passing through thesubintimal space, and thus improves the long-term results of the intervention.