
CASE20220817_003
Retrograde Recanalization of Chronic Occlusion of the Right Coronary Artery.
By , , , , ,
Presenter
Liudmila Ulyanova
Authors
1, 1, 1, 1, 1, 1
Affiliation
, Russian Federation1
Complex PCI - Chronic Total Occlusion
Retrograde Recanalization of Chronic Occlusion of the Right Coronary Artery.
1, 1, 1, 1, 1, 1
, Russian Federation1
Clinical Information
Patient initials or Identifier Number
Zh.B.N.
Relevant Clinical History and Physical Exam
Within 6 months, he notedcomplaints of anginal pain at level II F.C. Outpatient performed treadmill test - positive test. CAG was performedaccording to which: balanced type of blood supply. Stenosis in the middle segment of the LAD by80%, occlusion of the RCA at the proximal segment, occlusion of the OM at theostium. The first stage was performed stenting of PNA - DES 3.5*26 mm.
 cag lad.avi
cag lad.avi

cag rca.avi

lad.avi

Relevant Test Results Prior to Catheterization
Clinical blood test: RBC - 4.710 in 12 tbsp. / l; HGB - 147 g / l; MCV – 89.5 cubic meters; PLT - 183 10 in 9st. / l; MPV – 8.4 cubic meters; Leukocytes – 6.1 10 in 9 tbsp. / l/Biochemical blood test: Potassium - 4.44 mmol / l; Glucose – 9.96 mmol / L; GFR (MDRD) M – 99.61 ml / min / 1.73m2; Serum creatinine – 75.7μmol / l.
Relevant Catheterization Findings
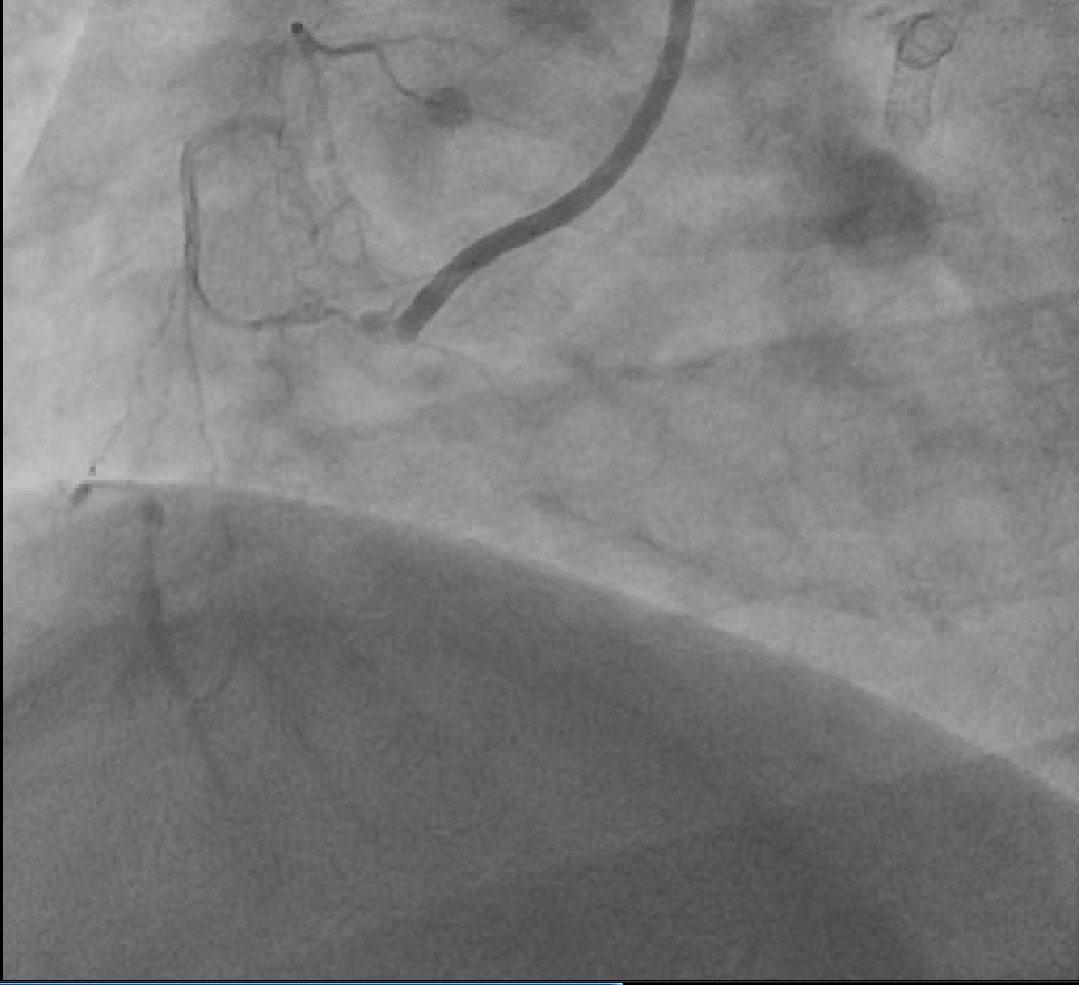
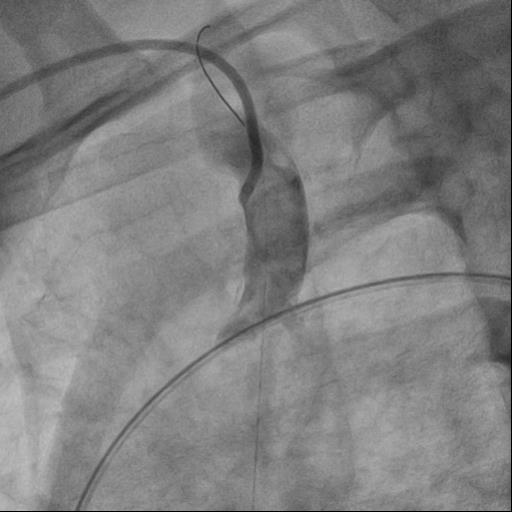
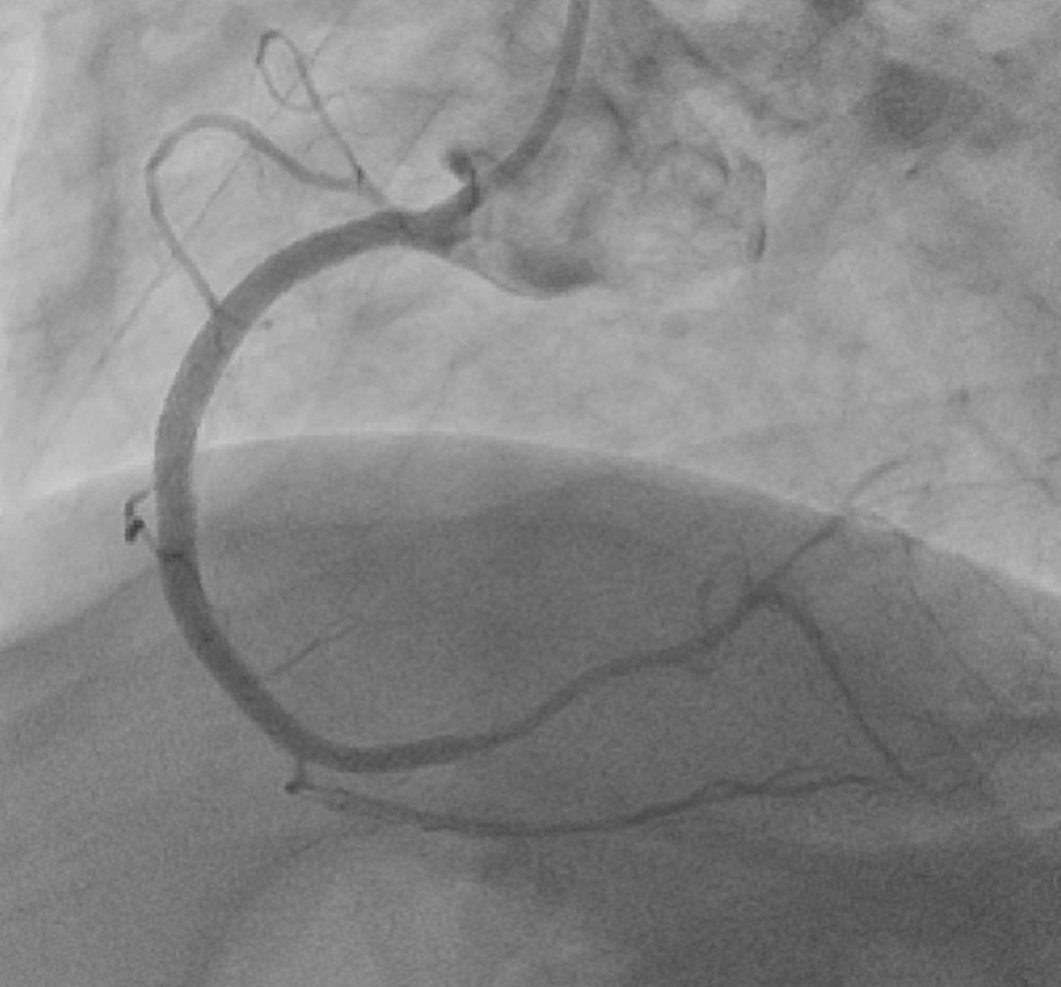
Type of coronary blood supply:balanced. LM: not changed. LAD: in the proximal and middle segments, a stentedarea is visualized, without signs of restenosis and thrombosis. LCx: withuneven contours. The OM at the ostium is occluded, the post-occlusion sectionis well filled along the intrasystemic collaterals. RCA: occluded in theproximal segment, post-occlusion section is well filled along intra- andintersystem collaterals.
lad.avi

rca.avi
Interventional Management
Procedural Step
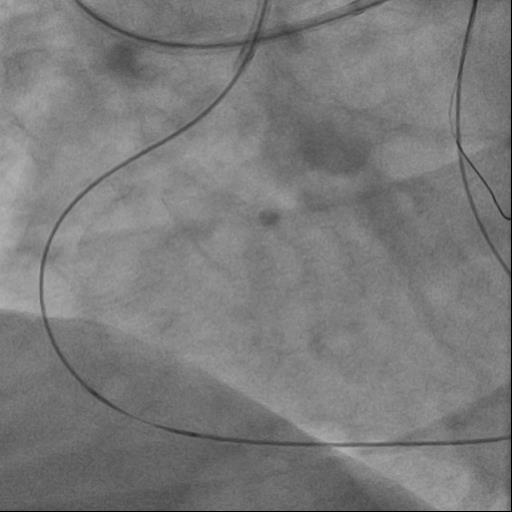
Attempts to antegradeconduction of wires of various stiffness into the true lumen of the artery wereunsuccessful. Performed retrograde recanalization of the RCA. Numerous attemptsto insert a retrograde wire into the antegrade catheter, at the ostium of theRCA, were unsuccessful. The retrograde wire was passed into the brachycephalictrunk and, with the help of a trap, was tightened into the antegrade catheter.An antegrade microcatheter was introduced into the distal channel along aretrograde wire. A 3.0-20 mm balloon catheter was used to predilate theaffected areas of the RCA. DES 2.75x20 mm, DES 3.5x38 mm, and DES 3.5x33 mm were implanted into the distal,middle, and proximal RCA segments at pressures of 14, 16, and 16 atm.respectively.
br.avi
f.avi
Case Summary
Recanalization of CTO is oneof the most complex interventions on the coronary arteries. When starting aprocedure, the operator must have several action plans. Knowledge andexperience, the availability of tools are the key to a successfulrecanalization result.