
CASE20220806_001
"Hanging By A Thread" - A Challenging Case of Acute Coronary Syndrome caused by Critically Stenosed Distal Left Main and critically stenosis Right Coronary Artery due to Eruptive Calcified Nodules in an Octogenerian Patient.
By ,
Presenter
Tjen Jhung Lee
Authors
1, 1
Affiliation
, Malaysia1
Complex PCI - Calcified Lesion
"Hanging By A Thread" - A Challenging Case of Acute Coronary Syndrome caused by Critically Stenosed Distal Left Main and critically stenosis Right Coronary Artery due to Eruptive Calcified Nodules in an Octogenerian Patient.
1, 1
, Malaysia1
Clinical Information
Patient initials or Identifier Number
461567
Relevant Clinical History and Physical Exam
We detailthe history of an 88 year old fit man withbackground hypertension and benignprostatic hyperplasia, planned for surgical treatment. A pre-operative Exercise stress ECHOshowed ST depressions with hypokinesia at the anterior segments at peakexercise.
Relevant Test Results Prior to Catheterization
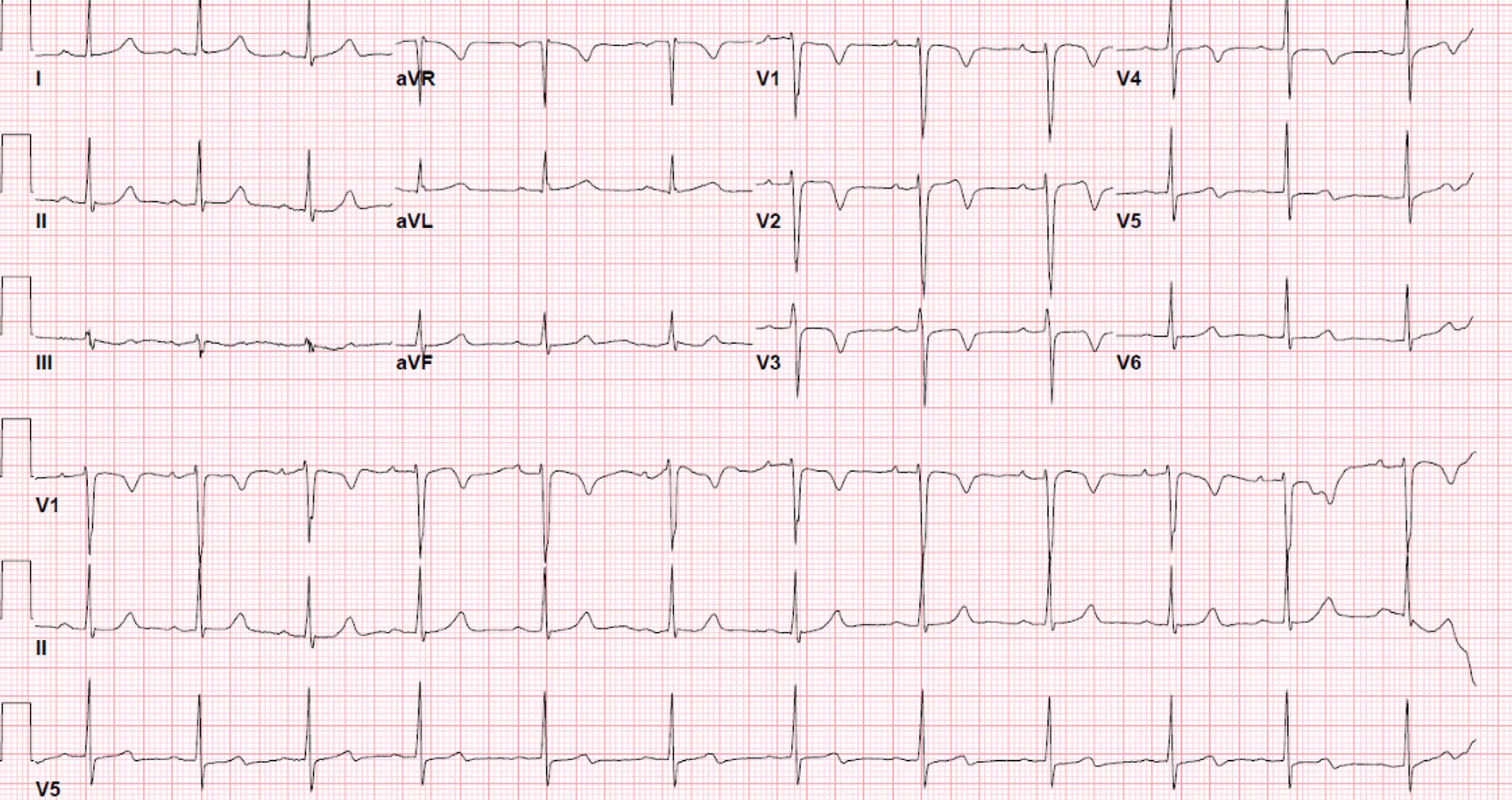
Electrocardiogram: T inversions in leads V1-V3 at rest
 ECHO2.avi
ECHO2.avi
Relevant Catheterization Findings
Invasive coronary angiogramLeft Main Stem (LMS): Critical 99% distal LMS stenosis caused by calcified nodule
Impression: Severe calcified 3 vessel disease
LMS pre.avi
LMS pre2.avi
RCA pre.avi
Impression: Severe calcified 3 vessel disease
Interventional Management
Procedural Step
Heart team meeting was held, and patient outright refused bypass surgery due to age-related peri-operative risks and background COPD. Thus high-risk multivessel angioplasty was done in two stages.
RCA post.avi
LMS post.avi
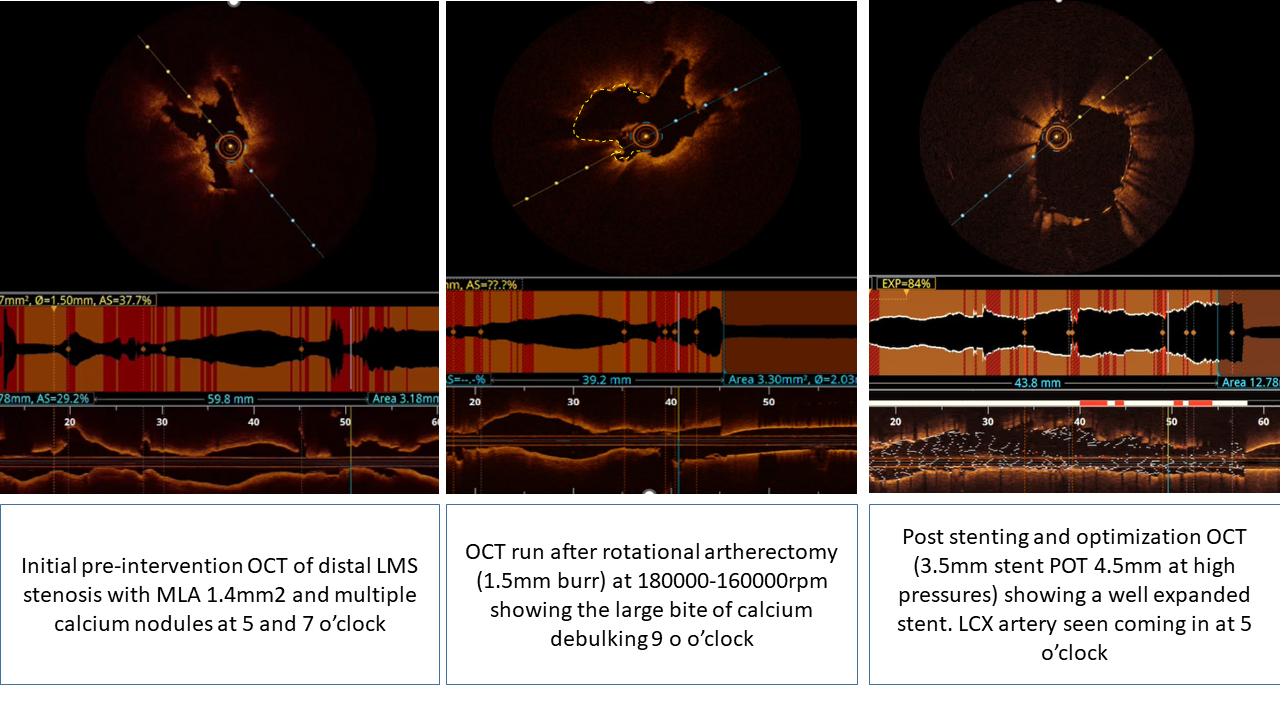
OCT 1st run before Rota.avi
OCT 2nd run after Rota.avi
OCT 3rd run after stent and optimization.avi
Case Summary
Patient recovered well post angioplasty and was discharged home the next day. He is well at 1 months clinic follow up with NYHA class 1 and no chest pain, and has returned to his usual routine of cycling.