
CASE20220805_002
Left Main stenting done with Provisional approach- Can Imaging with IVUS make a difference
By
Presenter
Rohit Mody
Authors
1
Affiliation
, India1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Left Main stenting done with Provisional approach- Can Imaging with IVUS make a difference
1
, India1
Clinical Information
Patient initials or Identifier Number
Case 1- 200697 Case 2- 230483 Case 3- 221292
Relevant Clinical History and Physical Exam
case 1- 79 Year old Male AOE 3 Chest Pain Dyslipidemic Case 2- 73 Year old Male Diabetic Hypertensive AOE 3 Case 3- 59 year old female Non Diabetic AOE 3 normal BMI, Hypertensive, Dyslipidemic and family history of CAD
Relevant Test Results Prior to Catheterization
Case 1- TMT possitive, Troponin possitive Case 2- Troponin possitive, TMT negative
Relevant Catheterization Findings
Case 1- Angiography Reveals DVD- LAD and LCX Diseased Case 2- Angiography reveals LM disease with LAD 90% & LCX 85% Case 3- Angiography reveals TVD

Interventional Management
Procedural Step
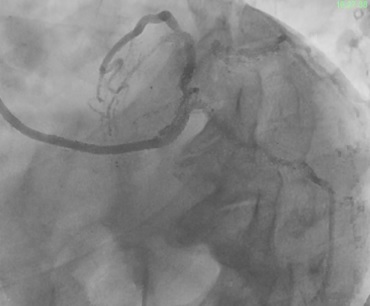
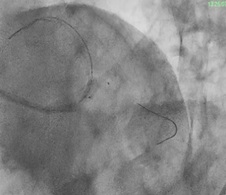
Case 1- LM Hooked with EBU 3.5 6F, LAD crossed with BMW wire & LCX with Floppy wire, 2.75x38mm DES In LAD at 14 ATM, 4.0x22mm DES in LM to LAD at 16 ATM, 2.5x12mm in LCX at 14 ATM, IVUS showed Under deployed stents KBT done with 2.5mm balloon in LCX & 3.5mm balloon in LM to LAD using TAP technique. Good Final results, no complications, TIMI 3 Flow achieved. Case 2- LM hooked with EBU 4.0 6F catheter crossed LAD & LCX with BMW wire, 3.5x28mm DES deployed in Mid LCX, 3.5x12mm DES deployed in Distal LCX, Pre-Dilatation done with 2x8mm balloon in LAD, 3.5x38mm DES deployed in mid to Distal LAD, 4.0x38mm DES deployed in Proximal to Mid LAD. Another 3.5x23mm DES deployed in LM to LCX at 14 ATM using TAP technique, KBT done with 3.5mm balloon in LM to LCX & 4mm in LAD, Good Final results achieved, no complications, TIMI 3 Flow achieved. Case 3- LM Hooked with JL 3.5 6F catheter, crossed the lesion with BMW wire, IVUs run was taken but unable to cross the tightest point. Pre-Dilatation done with 2.5x15mm Balloon and Dog boning was seen, 40 Pulses given in LAD using 3.0x12mm IVL catheter, 2.5x28mm DES deployed in Mid LAD, Another 3.0x22mm DES deployed in ostial LAD at 18 ATM, In LCX Pre-Dilatation done with 1.5x15mm Balloon, In LCX 40 pulses given with 2.5x12mm IVL catheter, 2.25x12mm DES deployed in mid LCX at 16 ATM, 2.5x18mm DES in proximal LCX at 16 ATM, Good final results achieved, no complication and TIMI 3 Flow achieved.

 21.avi
21.avi
22.avi
Case Summary
Multilayered Provisional strategy remains treatment of choice for Left Main Bifurcation Lesions. In Provisional stenting Second stent can be deployed is and when required There is a considerable role of IVUS Imaging and Physiology in optimizing the results and improving outcomes Kissing Balloon is an important step in LM Bifurcation strategy proper technique is important to prevent future side branch occlusion. Double kissing in various technique give better results. IVUS imaging can identify the underexpansion. Sync vision with Philips gives important information with clear dog boning and subsequent expansion of the stent.