
CASE20220801_001
I Wish I Had Done It Before Transcatheter Aortic Valve Replacement: Ostial Right Coronary Artery Intervention With Rotablation of a Calcified Lesion and Transcatheter Heart Valve Stent Struts Obstruction
By , ,
Presenter
Huan-Chiu Lin
Authors
1, 1, 1
Affiliation
, Taiwan1
Complex PCI - Calcified Lesion
I Wish I Had Done It Before Transcatheter Aortic Valve Replacement: Ostial Right Coronary Artery Intervention With Rotablation of a Calcified Lesion and Transcatheter Heart Valve Stent Struts Obstruction
1, 1, 1
, Taiwan1
Clinical Information
Patient initials or Identifier Number
6173203
Relevant Clinical History and Physical Exam
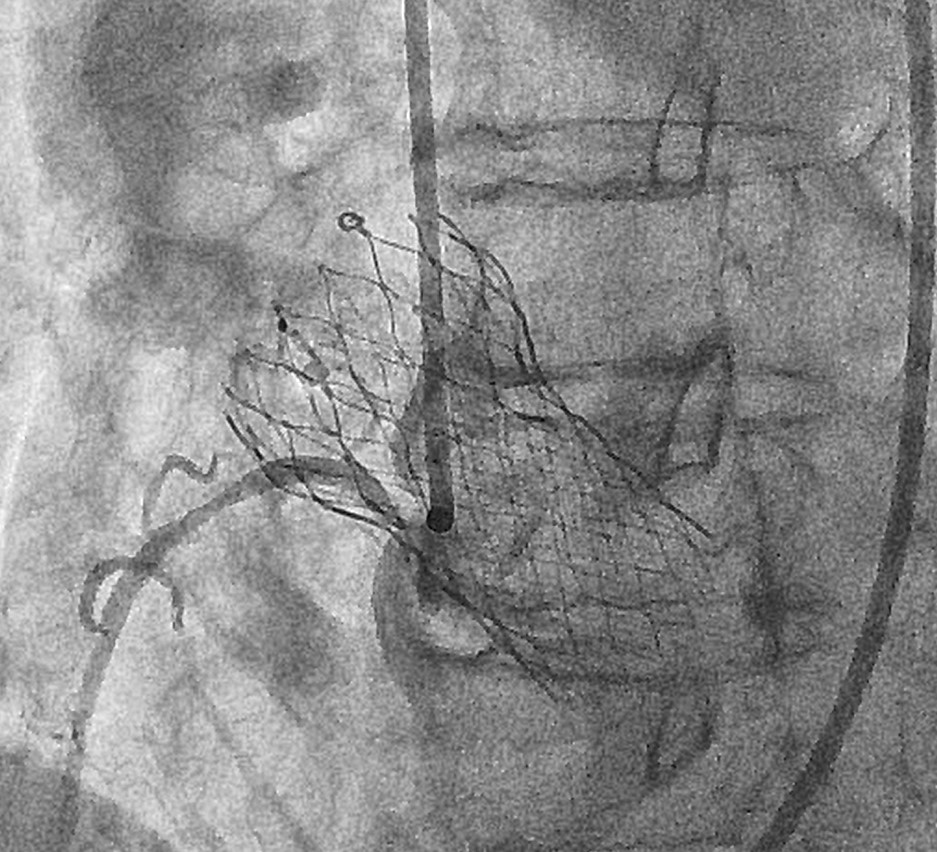
An 90-years-old woman with previous history of coronary artery disease with triple vessel disease, with a drug eluting stent at distal portion of left circumflex artery, Valvular heart disease with severe aortic valve stenosis, and recieved transcatheter aortic valve replacement with 26mm self-expanding bioprosthetic valve(Medtronic CoreValve Evolut PRO) in June, 2021.

 Video A.WMV
Video A.WMV
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
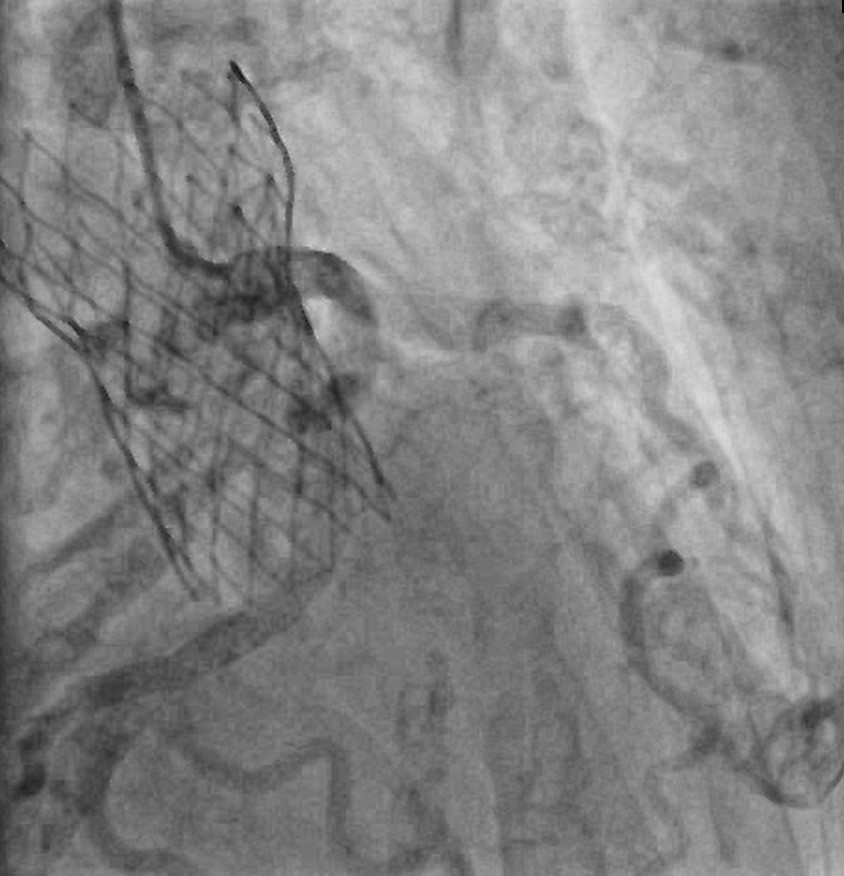
LM: PatentLAD: LAD-M 50% stenosis with calcificationLCX: Co-dominant LCX and RCA LCX-M 40% stenosis LCX-M to D stent patent LCX-OM2 and OM3 50% stenosisRCA: Co-dominant LCX and RCA RCA-ostium 70-80% stenosis with an acute angulation and heavy calcification RCA-P 70% stenosis
video A.WMV
video B.WMV
Interventional Management
Procedural Step
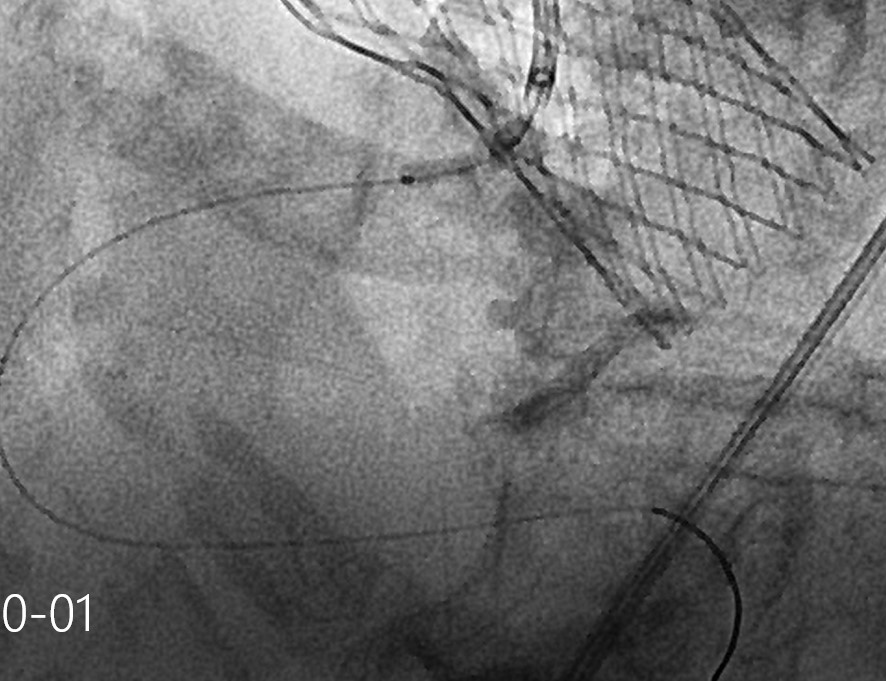
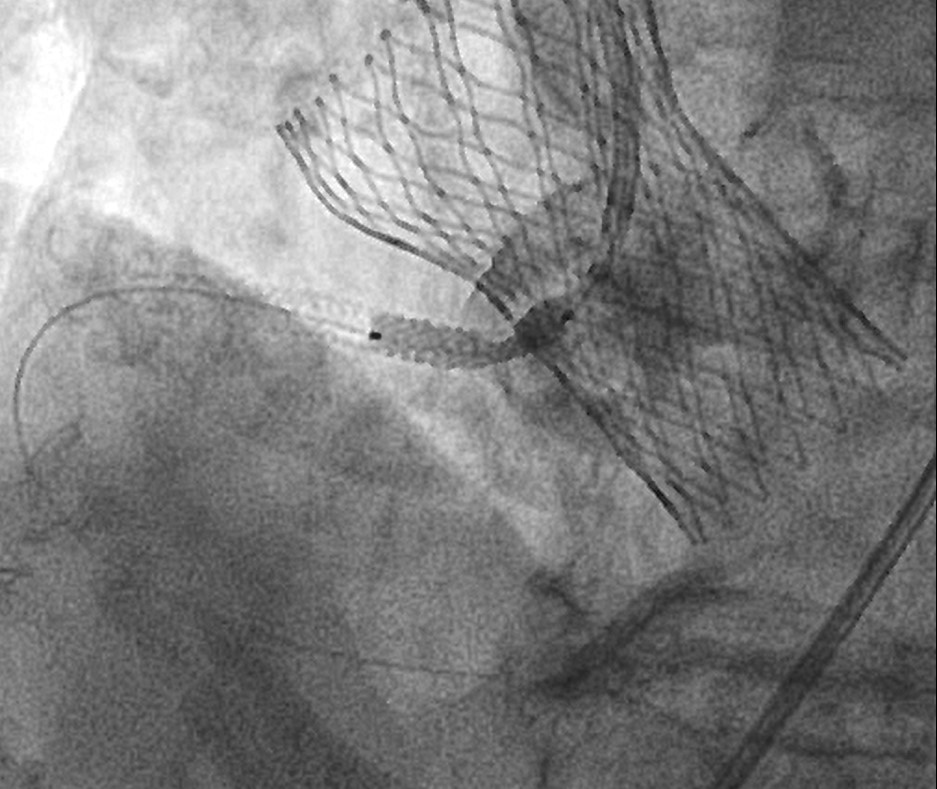
1.RCA was partial engaged with JR4(SH)/6F guiding catheter. 2.Sionblue wire to RCA-PDA, introduced Guideliner 5.5F.3.After POBA, confirmed a balloon undilatable lesion at RCA-ostium, and possible TAVR stent struts or remanent aortic valve obstruction at RCA-orifice.4.Changed to Rota wire(Floppy), and rotablation of RCA-ostium to RCA-P were performed with with 1.25mm Rota burr and 1.75mm Rota burr (high speed 160,000 rpm).5.Changed to workhorse wire.6.Sequential POBA with 2.0 x 12mm SC balloon and 2.5 x 12mm SC balloon at 8-12atm.7.IVUS showed two separated lesions at RCA-ostium and RCA-P, with heavy atherosclerotic plaque, near 360 degree of superfical calcium arc which was broken by Rotablation was noted at ostium. There was also a lesion between the TAVR struts and RCA-ostium, suspected remanent aortic valve. 8.A 3.5 x 38mm Synergy DES and a 4.0 x 16mm Synergy DES were deployed(overlapping at RCA-ostium to increase radial force, 2-3mm protrution into meshes of THV).9.Post-dilatation with 4.0 x 12mm NC balloon.10.The final angiogram result was optimal.

video A.WMV
video B.WMV
video C.WMV
Case Summary
Clinical suspicion and history of TAVR should be taken into account for early recognition of impending deplay coronary obstruction. Rotablation of calcified lesion at coronary orifice and transcatheter heart valve stent struts obstruction, with stent implantation through the meshes of the biological valve is a high risk and challenging procedure but can lead to a successful outcome.